General Information about Zudena
Zudena is available in varied strengths, ranging from 25mg to 200mg, allowing for individualized therapy depending on the severity of erectile dysfunction. The beneficial starting dose is 100mg, taken on an as-needed foundation, but this can be adjusted accordingly. The treatment shouldn't be taken greater than as quickly as a day.
Erectile dysfunction, also identified as impotence, is the inability to realize or preserve a firm sufficient erection for sexual activity. It is a widespread situation, especially amongst older men, and might have a significant impression on their high quality of life. In the past, the treatment for erectile dysfunction was restricted, with options similar to penile implants and vacuum pumps being the primary choices. However, with the development of PDE5 inhibitors, males with erectile dysfunction now have more remedy choices, with Zudena being the most recent addition.
Udenafil is also well-tolerated and protected for most males. Common unwanted effects, corresponding to headache, flushing, stuffy or runny nose, and dizziness, had been reported to be mild and momentary. However, as with any medicine, it is essential to seek the assistance of a physician before beginning remedy with Zudena, as it might interact with different medicines or have adverse results in people with certain medical situations. Men who are taking nitrates or alpha-blockers for heart situations shouldn't take Zudena as it can lead to a dangerous drop in blood stress. Therefore, a thorough medical evaluation is important to make sure the safety and effectiveness of the medication.
One of the primary advantages of Zudena over other PDE5 inhibitors, such as Viagra and Cialis, is its longer period of action. While the effects of Viagra and Cialis final for around 4-6 hours, Zudena can provide an erection for up to 12 hours. This means that a person can take the treatment and have interaction in sexual activity each time they want inside that time-frame, without worrying concerning the effects carrying off. This added flexibility makes Zudena a popular choice amongst males with erectile dysfunction.
In conclusion, Zudena (Udenafil) is a promising addition to the therapy choices for erectile dysfunction. With its longer duration of motion, fast onset, and good security profile, it has quickly gained reputation amongst males with this condition. However, as with all medicine, it's crucial to use it underneath the steerage of a healthcare professional to ensure its secure and efficient use. With Zudena, men with erectile dysfunction can regain their confidence and improve their sexual relationships, leading to a greater high quality of life.
Zudena, also referred to as Udenafil, is a medication that has gained attention within the field of urology for its use in treating erectile dysfunction. This drug is a member of the category of phosphodiesterase kind 5 (PDE5) inhibitors, which work by rising blood circulate to the genital space, resulting in an erection. It was accredited by the United States Food and Drug Administration (FDA) in 2018, changing into the most recent addition to the list of medicines used to manage erectile dysfunction.
Another advantage of Zudena is its speedy onset of action. It sometimes begins working within 30 minutes, making it a suitable choice for spontaneous sexual activity. This makes Zudena different from other PDE5 inhibitors, which can take up to an hour to take impact. This convenience is especially helpful for males who need to plan their sexual activity around their medication consumption.
The cleft mitral valve is best demonstrated in the parasternal short-axis view at the level of the mitral valve problems with erectile dysfunction drugs zudena 100 mg buy without a prescription. While cardiac surgery has been questioned in children with Down syndrome based upon past surgical results or the long-term natural history and survival of this population, more recent data demonstrate that complete biventricular repair yields substantial benefits. Actuarial survival was 94 percent among the patients with Down syndrome versus 86 percent in the group with a normal karyotype. The presence of unbalanced ventricles was the only independent risk factor affecting survival in a multivariate analysis (p < 0. The explanation for these findings appears to be due to the higher prevalence of abnormalities of the mitral valve (4. Primary repair should be performed within the first 6 months, because of the early development of pulmonary vascular disease in unoperated patients with Down syndrome. In this retrospective study, 50 patients who were over the age of 18 years underwent 57 surgeries between 1969 and 2008, at a mean age of 33 years. This study showed that at an experienced center, adults with Down syndrome can undergo cardiac surgery with a low risk of early mortality (2%) and an acceptable morbidity, with atrial arrhythmias occurring in 25 percent and early postoperative pulmonary infections in 11 percent. Pulmonary artery thrombosis and emboli can occur in those with enlarged pulmonary arteries. Deep venous thrombi are less likely to cause paradoxical emboli, because the inferior vena caval flow is directed to the midportion of the inter-atrial septum (rather than the lower end, where the ostium primum defect resides). A licensed clinical social worker can help the family navigate through the medical system and can furnish information regarding schools and training programs for these children. Such programs help provide growing children with the skills required to deal with activities of daily living, as well as to direct them to vocations that offer community involvement, reimbursement and a sense of accomplishment which promotes self-esteem. Support programs also provide an opportunity for parents and grandparents to interact with other families in similar circumstances. There are several national and international organizations which are driven by families of individuals born with Down syndrome. Major organizations in the United States include the National Association for Down syndrome ( Additional programs offer parental workshops, medical in-service, psychosocial services, mentoring, public awareness, internet-based discussion forums and newsletters. Regional and national organizations in other countries can establish programs based on this model to offer resources appropriate for the needs of their local population. There are several books on the subject of Down syndrome available online or can be obtained at a local book store or library. For females with Down syndrome, the transition may start earlier, since there is a need to discuss contraception and sterilization with the patient and her family at menarche and implement these actions following informed consent from the parents or guardians. There are concerns that females with Down syndrome, based on their intellectual development, may be challenged to care for their offspring. Pregnancy on its own can pose hemodynamic strain in females born with congenital heart defects and, in particular, carries a higher risk in those with pulmonary vascular disease. Limited longevity and other co-morbidities such as early onset of Alzheimer disease may also limit the ability of women with Down syndrome to care for their offspring, thus adding to the list of ethical dilemmas in allowing them to procreate. Most children with Down syndrome have health complications beyond the usual childhood illnesses (Box 1). Box 1: risk-factors for morbidity and mortality in Down syndrome · Congenital heart defects · Respiratory tract infections · Gastrointestinal tract congenital defects · Hepatitis B virus · Hematological issues: leukemia · Endocrine disorders: hypothyroidism · Immunological disorders · Premature Alzheimer disease Around 45 to 50 percent have congenital heart defects. It is imperative that an echocardiogram be performed on all newborns with Down syndrome in order to identify any serious cardiac problems that might be present. Some of the heart conditions require surgery, while others only require careful monitoring. These patients also have a higher incidence of comorbidities such as upper and lower respiratory infections, impaired vision, hearing problems and thyroid disorders, among other medical conditions. The American Academy of Pediatrics no longer advises routine lateral cervical spine X-rays in flexion and extension at the ages of 3 to 5 years, 12 years, and 18 years for the diagnosis of atlantoaxial instability. They should be reminded about maintaining adequate hydration, eating a balanced diet and performing regular exercise. Information should be provided about routine dental/skin care and bacterial endocarditis prophylaxis before dental cleaning. In patients over 35 years of age, screening for Alzheimer disease should be performed. Unoperated adults who develop pulmonary hypertension with or without cyanotic congenital heart defects need additional medical management. Appropriate medical and surgical care can lead to an improved quality of life in most children and adults with Down syndrome. Currently, the average life expectancy of individuals with Down syndrome is 55 years, but may increase with early surgical intervention and medical care. Germinal and somatic trisomy 21 mosaicism: how common is it, what are the implications for individual carriers and how does it come about Atlantoaxial instability in individuals with Down syndrome: epidemiologic, radiographic, and clinical studies. The problem of mitral insufficiency caused by accessory chordae tendinae in persistent common atrioventricular canal. The presence of Down syndrome is not a risk factor in complete atrioventricular septal defect repair. Does Down syndrome affect prognosis of surgically managed atrioventricular canal defects In this chapter, our objective would be to learn the answers for this pertinent question to the best of current knowledge. The possible cause of the defect may lie anywhere from genes to drugs or diseases affecting the embryogenesis. The diagnostic advances achieved to date still fall short of unearthing the precise cause of congenital heart diseases in all cases. Some of the tests are so sophisticated that they are yet to come out of research laboratories! Added to the woes are lack of trustworthy regional epidemiological data to understand the interaction between various possible causes and how they work in tandem or independently.
Cysts Sebaceous cyst: the common site for sebaceous cyst is postauricular sulcus below and behind the ear lobule impotence causes and treatment zudena 100 mg order line. Etiology: the radiation and chronic ear inflammation are the two important etiologic factors. Clinical features: They present as smooth, sessile, bony swellings in the deeper part of the bony meatus near the tympanic membrane. Keloid of auricle the common sites for keloids, which occur after trauma or piercing of the ear for ornaments, are the lobule or helix. Recurrence after surgery of keloid that occurred after ear piercing 270 Squamous Cell Carcinoma of auricle Clinical features Box 1: tumors of the middle ear and mastoid · Benign Glomus tumor: Glomus jugulare and glomus tympanicum · Malignant Primary Carcinoma: Squamous cell carcinoma, adenocarcinoma Sarcoma: Rhabdomyosarcoma, osteosarcoma, lymphoma, fibrosarcoma and chondrosarcoma Secondary Metastatic: Carcinoma of bronchus, breast, kidney, thyroid, prostate and gastrointestinal tract From adjacent areas: Nasopharynx, external auditory canal and parotid Predisposing factor: Prolonged exposure to direct sunlight. Treatment In small lesion with no nodal metastasis, local excision with 1 cm of safety margin is sufficient. Clinical features: Nodular ulcer with raised or beaded edge and central crust, which on removal result in bleeding. Though the tumor is locally invasive, its growth is very slow, extending over several years. Glomus Tympanicum: this tumor arises from the promontory and may cause facial paralysis. Advanced lesion: Superficial melanoma (larger than 1 cm), infiltrative melanomas, melanoma of posterior auricular surface or concha and recurrent melanomas need resection of pinna, parotidectomy and radical neck dissection. Spread Local: the tumor first fills the middle ear and then invades the tympanic membrane and present as an ear polyp, which bleeds readily. Red, vascular polyp filling the meatus, which bleeds readily and profusely on manipulation. Pulsatile tinnitus: In cases of pulsatile tinnitus, always first rule out the paraganglioma (glomus tympanicum or jugulare). The aberrant carotid artery, high or dehiscent jugular bulb can also be diagnosed. Its indications are as follows: Inoperable tumors Residual tumors Recurrences after surgery Older patients who cannot withstand extensive skull base surgery. Differential Diagnoses Because of their appearance, glomus tumors may be mistaken for: High-riding jugular bulb or dehiscent jugular bulb. It arises either primarily from middle ear or is an extension of carcinoma of deep bony meatus. Enlargement of regional lymph nodes: Preauricular, postauricular, infra-auricular and upper deep cervical. Adenocarcinoma, which is less common, arises from the glandular elements of middle ear. Spread Treatment It consists of en bloc wide surgical excision with postoperative radiation. Surgery: Depending on the extent of tumor, it may consist of radical mastoidectomy, subtotal/total petrosectomy. The tumor destroys ossicles, facial canal, internal ear, jugular bulb, carotid canal, deep bony meatus and mastoid. An ulcerated area in the meatus or a bleeding friable polypoid mass or granulations. Tumors of the ear and Cerebellopontine angle Growth Acoustic neuroma arises from the Schwann cells of the vestibular nerve twice as often as from the cochlear nerve. Difficulty in understanding speech is out of proportion to the pure tone hearing loss. Sudden-onset rotatory vertigo is rare because slow growth of tumor results in vestibular compensation. Cerebellum Finger-nose test, knee-heel test, dysdiadochokinesia, ataxic gait, inability to walk along a straight line with tendency to fall to the affected side. Roll over phenomenon (reduction of discrimination score when loudness is increased beyond a particular limit) is commonly observed. Chapter 25 w Tumors of the ear and Cerebellopontine angle Caloric test Diminished or absent response in 96% of patients. Disadvantages: Neurotologists less familiar with surgical anatomy of the area; Cochlea, semicircular canals and temporal lobe limit the exposure. Common sites are carotid bifurcation, jugular foramen and promontory of middle ear. During otoscopy with pneumatic speculum, on raising the pressure red mass behind the drum pulsates vigorously while reverse occurs on releasing the pressure. The earliest extracanalicular cranial nerve to be involved is trigeminal (especially sensory fibers affecting the corneal reflex). Anterior rhinoscopy allows assessment of nasal cavity, septum and inferior turbinate. Pain in cases of ethmoidal sinusitis is near the medial canthus and side of the nose. Cacosmia (perception of putrid odor) is common in cases of empyema of maxillary sinus. Box 1 shows the general format of examination of nose and paranasal sinuses and causes of common findings. Superficial ulcers and inflammation: It can be secondary to nasal discharge or due to herpes simplex. In patients with bilateral nasal stuffiness, it is important to know whether obstruction occurs simultaneously or alternately. In children, a unilateral purulent blood stained nasal discharge is usually due to foreign body unnoticed by parents.
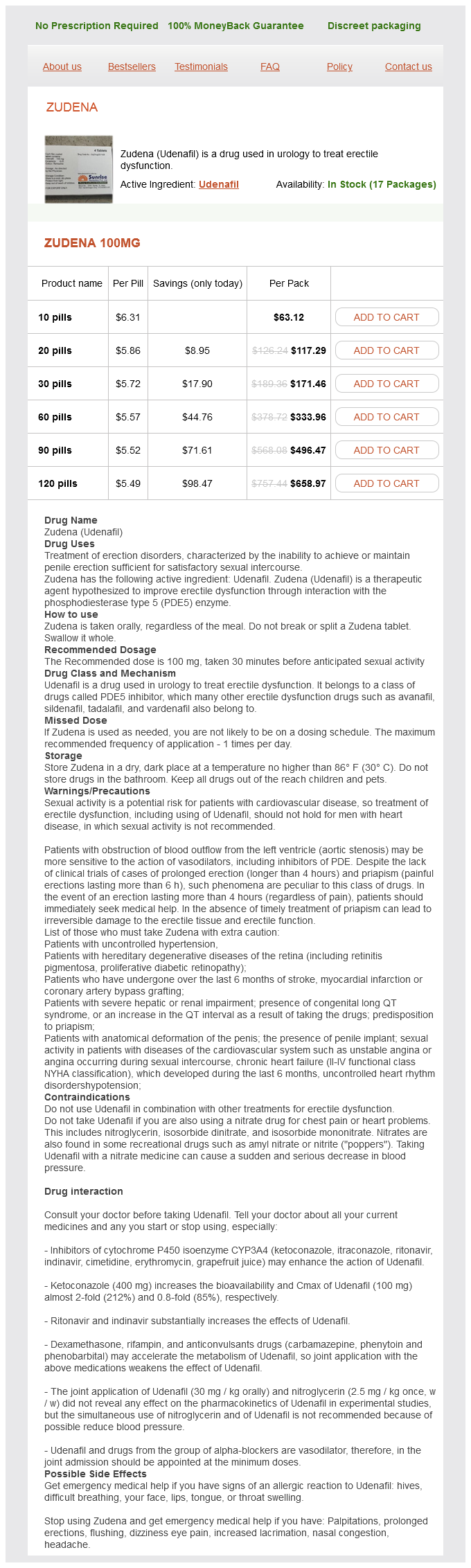
Zudena Dosage and Price
Zudena 100mg
- 10 pills - $63.12
- 20 pills - $117.29
- 30 pills - $171.46
- 60 pills - $333.96
- 90 pills - $496.47
- 120 pills - $658.97
Heavy infections can result in prolapsed rectum erectile dysfunction doctor karachi discount zudena 100 mg line, and growth retardation and finger clubbing may occur in children. Again, note that the head is found at the tiny end, and the expanded body of the worm contains the reproductive organs. They are passed unembryonated, measure 50-55 x 20-25 micrometers, are often tan, brown, or golden in color, and have very distinct polar plugs at either end. These are small worms, alternating between a free-living and parasitic life cycle. Adult males are usually only found in the soil and parthenogenic females occur both in the soil and in the small intestine. The eggs produced by the female are so thin walled that they normally rupture, releasing the free 1st stage (rhabditiform) larvae in the feces. Larvae are 300-380 micrometers long, colorless when unstained, with a short buccal cavity and pointed tail. Although more common in Europe and Asia, Ancylostoma duodenale (old world hookworm) is also found in North America and other portions of the Western hemisphere. The anterior margin of the buccal capsule has two ventral plates, each with two large cutting teeth fused at the bases. Because virtually all specimens are poorly oriented and the teeth cannot be clearly seen, you do not have to distinguish genera of hookworms from one another on sight. However, you should know the differences on the lab exam if I specifically state whether a particular specimen has teeth or cutting plates. Hint: be careful not to confuse the copulatory bursa of the male with the mouth region. The most common hookworm of the Americas is Necator americanus (new world hookworm). Because many specimens are poorly oriented so that the plates are not clearly seen, you do not have to distinguish genera of hookworms from one another on sight. However, as stated above, you should know the differences between the two genera if I state whether a particular specimen has teeth or cutting plates. The eggs of hookworms cannot easily be distinguished from one another by a novice. They are fairly thin walled and in the morula stage (generally the 4, 8, 16, or 32 cell stage). The walls of many hookworm eggs appear to have been dissolved during specimen processing (at least with our slides) and, thus, may be difficult to discern initially. The easiest way to find these eggs is to scan your slide using a 10x objective lens (100x total magnification) and identify the morulas. Then, switch the objective to 40x (400x total magnification) to better see the egg wall. Eggs are easily distinguished because they are subspherical and possess a thick, mammillated wall. You should be able to distinguish 3 types of eggs: 1) a fertilized egg with the mammillated wall; 2) a fertilized egg where the rough outer wall has been strippped away; and 3) an unfertilized egg which is generally longer and narrower than fertilized ones, the internal details appear as disorganized globules, and and the inner chitinous and lipid wall layers are not formed. These larvae are microscopic L1 stages that can be seen coiled within individual skeletal muscle cells. The technically correct name for this species is Calodium hepaticum, although few textbooks have yet made the conversion. Adults are found in the liver, although it is unlikely that you will see a cross-section through one. The female produces numerous eggs that are retained and encapsulated within the liver parenchyma. Eggs are similar to Trichuris in that they have bipolar plugs in either end, however, they tend to be more squared off at the ends than Trichuris. Once the eggs are liberated into the environment, either by passing through the gut of a carnivore or following host decomposition, eggs embryonate and become infective. Related species known to infect humans and for which eggs may be found in human feces include Aonchotheca philippinensis (Capillaria philippinensis), an intestinal parasite normally using a bird/fish life-cycle, and Eucoleus aerophilus (Capillaria aerophilus), a respiratory tract parasite of carnivores. Adults live in subcutaneous nodules and produce microfilariae that wander throughout the skin. These larvae are unsheathed (without an embryonic membrane) and have a tapered, flexed tail. Adults of the first two species live in lymphatics and produce microfilariae that circulate in the bloodstream. Adults of Loa loa wander throughout the dermis and produce microfilariae that also enter the bloodstream. Larvae of all species have an embryonic sheath, tapered tail, and are difficult to tell apart without a good stain. Based on the above information and that in your text, you should know the following key characters for differentiating Onchocerca volvulus, Wuchereria bancrofti, Brugia malayi, and Loa loa: 1) Whether the microfiliariae are sheathed or non-sheathed. Demonstration: Know how to distinguish female Ascaris lumbricoides (large; straight tail) from males (smaller; hooked tail). Demonstration: Dioctophyma renale are the largest of the worms you will be examining. Adults occur in the kidneys, and eggs with bipolar plugs somewhat like Capillaria hepatica pass out with the urine. Females are much larger than males, and do not have the copulatory bursa of the male.
© 2025 Adrive Pharma, All Rights Reserved..