General Information about Zofran
In conclusion, Zofran is a extremely efficient medicine used to forestall nausea and vomiting in patients undergoing cancer therapy or surgical procedure. It works by focusing on serotonin receptors within the physique, decreasing the nerve indicators that trigger these signs. While it may cause some unwanted effects in some individuals, the benefits of this medicine outweigh the potential risks, making it a useful device in the administration of nausea and vomiting. If you would possibly be experiencing these symptoms because of chemotherapy or surgical procedure, discuss to your doctor about whether Zofran is a suitable possibility for you.
In addition to its use in most cancers patients, Zofran is also useful for sufferers who undergo surgical procedure. Surgery, no matter its sort, could be a annoying experience for the body, and it is not uncommon for sufferers to expertise nausea and vomiting after recovering from anesthesia. Zofran can be administered before surgical procedure to help prevent these symptoms from occurring, making the post-operative restoration process extra comfortable for the patient.
While Zofran is usually well-tolerated, like all medication, it could trigger side effects in some people. The commonest unwanted effects of Zofran embrace headache, dizziness, constipation, and fatigue. These side effects are often gentle and short-term, and most sufferers don't experience any vital points while taking this medication. However, it's essential to tell a healthcare supplier if any severe or persistent side effects happen.
There are various types of Zofran out there, together with tablets, oral disintegrating tablets, and injectable solutions. The dosage and method of administration will depend upon the affected person's medical situation and individual needs. It is essential to take Zofran as directed by a healthcare skilled and follow the prescribed dosage fastidiously.
One of the primary uses of Zofran is in most cancers sufferers who're receiving chemotherapy. Chemotherapy is a typical type of most cancers treatment that entails using highly effective medication to kill cancer cells. While chemotherapy can be efficient in preventing most cancers, it also comes with a range of side effects, some of the significant being nausea and vomiting. These side effects can be debilitating and may have a significant impression on a affected person's quality of life. Zofran is often prescribed alongside chemotherapy to help stop these symptoms and permit sufferers to proceed their remedy with out interruption.
In rare instances, Zofran might cause a potentially serious side effect referred to as serotonin syndrome, which might occur when there is an extra amount of serotonin within the physique. Symptoms of serotonin syndrome include confusion, agitation, muscle stiffness, fever, and irregular heartbeat. If any of these signs happen, it's crucial to seek medical consideration immediately.
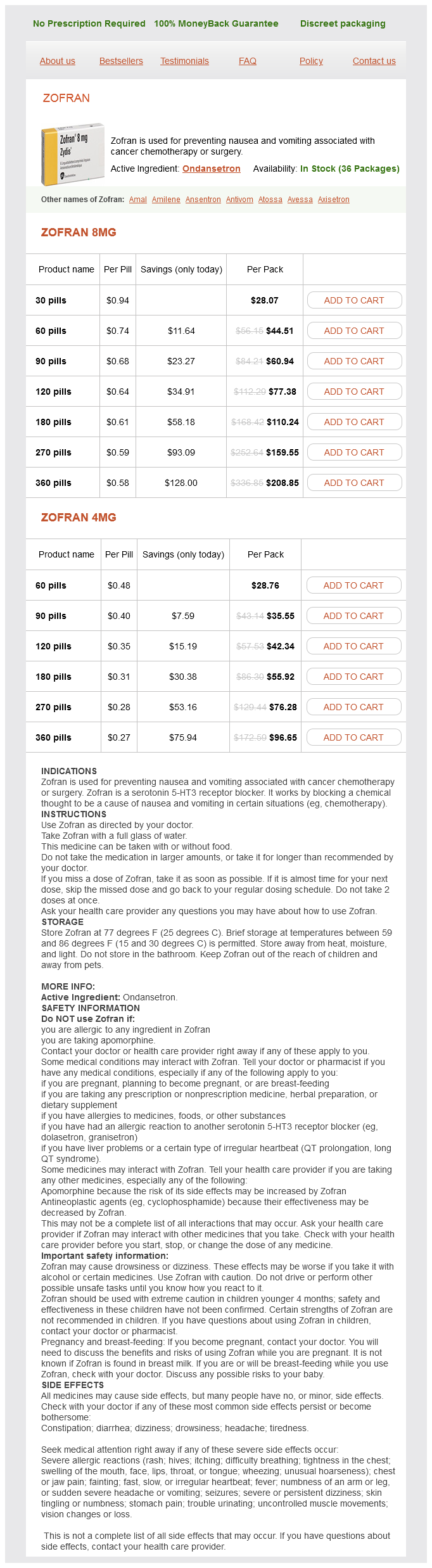
Zofran is a medication generally used in the prevention of nausea and vomiting attributable to certain medical remedies, such as cancer chemotherapy and surgery. It belongs to a class of medicine often known as antiemetics, which work by blocking the actions of chemical compounds within the body that may set off nausea and vomiting. This treatment has been a game-changer for so much of patients present process cancer remedy or surgical procedure, because it helps to reduce the uncomfortable and ugly side effects of these procedures.
Zofran works by blocking the actions of serotonin, a chemical in the physique that can set off feelings of nausea and vomiting. This treatment targets serotonin receptors within the gut and the brain, helping to reduce the nerve signals that cause nausea and vomiting. By doing so, Zofran successfully helps to prevent these symptoms, providing aid to sufferers present process chemotherapy or surgery.
Older children medications while pregnant buy discount zofran online, however, become unwell, and young adults develop infectious mononucleosis or glandular fever 47 weeks after initial infection. Hepatitis may occur, with mild elevations of hepatocellular enzymes in 90% of cases and jaundice in 9%. These include aseptic meningitis and encephalitis, nearly always with complete recovery, haemolytic anaemia, airway obstruction due to oropharyngeal swelling, haemophagocytic syndrome and splenic rupture. The symptoms are presumably due to the action of cytokines released during the intense immunological activity. The infected B cells are stimulated to differentiate and produce antibodies; this polyclonal activation of B cells is responsible for the production of heterophil antibodies (reacting with erythrocytes of sheep or horses) and a variety of autoantibodies. Spontaneous recovery usually occurs in 23 weeks, but the symptoms may persist for a few months. About 1% of cases develop an autoimmune haemolytic anaemia, which subsides within 12 months. These are present in 90% of cases, but may not be detected in those less than 14 years of age and the response is also short lived. In immunosuppressed people in specific clinical settings there are some data on using specific antivirals to reduce viral replication, but they are effective only in the lytic part of the life cycle. The subunit vaccine was shown to have a significant effect on clinical disease but did not prevent infection. EpsteinBarr virus remains latent in a small proportion of B lymphocytes EpsteinBarr virus is well equipped to evade immune defences (see Ch. This inherited disorder involves mutations in the gene that codes for the signalling lymphocyte activation-molecule-associated protein. Therefore, individuals with this X-linked disorder can develop fatal infectious mononucleosis and lymphomas and these can be prevented only by having an allogeneic bone marrow transplant. Each of these types of bacteria attach to the mucosal surface, sometimes invading local tissues. The rash begins as facial erythema and then spreads to involve most of the body except the palms and soles. The rash fades over the course of 1 week and is followed by extensive desquamation. The skin lesions themselves are not serious, but they signal infection by a potentially harmful streptococcus, which in pre-antibiotic days could sometimes spread through the body to cause cellulitis and septicaemia. Antibodies formed to antigens in the streptococcal cell wall cross-react with the sarcolemma of the heart, and with tissues elsewhere. Chorea is an involuntary movement disorder and disease of the central nervous system resulting from streptococcal antibodies reacting with neurones. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography a scientific statement from the American Heart Association. In many resource-poor countries, rheumatic heart disease is the most common type of heart disease, seen where there is poverty and overcrowding. Immune cells are recruited and cytokines and chemical mediators produced, together with local complement and coagulation systems being activated, resulting in inflammation in the glomeruli. Blood appears in the urine (red cells, protein) and there are signs of an acute nephritis syndrome (oedema, hypertension) 12 weeks after the sore throat. Understanding the pathogenesis of this infection helps to explain the disease picture, sites of shedding and the complications that can arise. Diagnosis A laboratory diagnosis is not generally necessary for pharyngitis and tonsillitis There are many possible viral causes of pharyngitis and tonsillitis, and the clinical condition is generally not serious enough to seek laboratory help. Although during the winter months up to 16% of schoolchildren carry group A streptococci in the throat without symptoms, treatment is recommended. However, susceptible adults are at risk of complications of mumps such as orchitis. After entering the body, the primary site of replication is the epithelium of the upper respiratory tract or eye. The virus spreads, undergoing further multiplication in local lymphoid tissues (lymphocytes and monocytes) and reticuloendothelial cells. Infected cells lining the parotid ducts degenerate and finally, after an incubation period of 1618 days, the inflammation, with lymphocyte infiltration and often oedema, results in disease. This is the classic sign of mumps, and parotitis is the most common clinical sign. Other sites may be invaded, with clinical consequences such as inflammation of the testis and pancreas, resulting respectively in orchitis and pancreatitis (Table 19. Close contact is necessary, for Treatment and prevention There is no specific treatment, but mumps is prevented by using the attenuated live virus vaccine, which is safe and effective. These rates had improved by 2017: in the United Kingdom the coverage was above 90%. The range of secondary bacterial invaders is the same as for other upper respiratory tract infections. Blockage of the eustachian (auditory) tube or the opening of sinuses, caused by allergic swelling of the mucosa, prevents mucociliary clearance of infection, and the local accumulation of inflammatory bacterial products causes further swelling and blockage. A study in Boston showed that 83% of 3-year-olds had had at least one episode, and 46% had had three or more episodes since birth. There may be general symptoms, and acute otitis media should be considered in any child with unexplained fever, diarrhoea or vomiting. The clinical diagnosis is confirmed by isolating bacteria from the blood and possibly the epiglottis. Respiratory obstruction due to diphtheria (see below) is rare in resource-rich countries, but the characteristic false membrane and local swelling can extend from the pharynx to involve the uvula. Most uncomplicated infections resolve with oral analgesics, but if there is no improvement then systemic antibiotics should be started. If acute attacks are inadequately treated, there may be continued infection with a chronic discharge through a perforated drum and impaired hearing.
Although vaccine-associated paralytic polio only occurs in <1 / million vaccinated treatment 1860 neurological zofran 8 mg order free shipping, vaccine-derived polio viruses can circulate within the community. Rubella vaccine the current rubella vaccine is a live attenuated virus, strain 27 / 3, licensed in 1979. The virus was attenuated by 2530 cell culture passages in human diploid fibroblasts. Over 90% of those vaccinated have at least 15 years of protection from clinical rubella or viraemia. Although rubella itself is a relatively mild infection, it causes real problems if pregnant woman become infected in the first trimester of pregnancy, when congenital rubella syndrome can cause serious damage to the fetus. Thankfully, there has been a dramatic reduction in confirmed cases of congenital rubella syndrome due to vaccination: cases fell by 98% in the Americas between 1998 and 2009. In 2016, only three countries reported cases of polio Afghanistan, Pakistan and Nigeria. Pneumococcal vaccines the challenge in making an effective vaccine against pneumococcal disease is that there are 90 serotypes of Streptococcus pneumoniae but luckily a few serotypes cause most infections. The first vaccine was a pneumococcal polysaccharide vaccine with capsular polysaccharide from 14 serotypes. However, although this vaccine induced antibodies in >80% of adults, it was not immunogenic in children aged less than 2 years. Animal studies have suggested that attenuated whole bacteria, or specific proteins from Strep. Giving the vaccine on sugar lumps or directly into the mouth was much easier than giving it by injection and the live vaccine also gives better intestinal immunity. The progress towards the eradication of polio is illustrated by the increase in certified polio-free countries from 1988 (top map) to 2016 (bottom map). Similar to the pneumococcal polysaccharide vaccine, the meningococcal polysaccharide vaccine was not immunogenic in young children, as for other T-independent antigens. The B strain is not included in either of these vaccines, as the B-group polysaccharide is poorly immunogenic and may have some cross-reactivity to the human nervous system. Haemophilus influenzae type b (Hib) Haemophilus influenzae mainly affects children under 5 years of age. Elimination of Haemophilus influenzae type b [Hib] disease from the Gambia after the introduction of routine immunisation with a Hib conjugate vaccine: a prospective study. Conjugating the polysaccharide to a T-cell-dependent antigen such as tetanus toxoid, diphtheria toxoid or the meningococcal group B outer membrane protein complex overcame this problem. Even so, three or four doses are needed to induce good immunity, as this is another example of how a subunit vaccine is less immunogenic than a live vaccine. Influenza Flu generated a lot of alarm in 2009, when the first flu pandemic since 1968 was caused by a new influenza A (H1N1) virus. The threat from this new virus, and from avian influenza (H5N1), highlighted the limited world capacity to produce new flu vaccines quickly in the quantities needed. Two types of vaccine are currently available: trivalent or quadrivalent inactivated vaccines that can be given to anyone over the age of 6 months by intramuscular or intradermal injection, and a live attenuated influenza vaccine given by intranasal spray to those aged 249 years of age who are healthy and not pregnant, that replicates in the mucosa of the nasopharynx. The 2016 / 2017 trivalent vaccines for the northern hemisphere contained A/California/7/2009 (H1N1)-like, A/Hong Kong/4801/2014 (H3N2)-like and B/ Brisbane/60/2008-like antigens. The influenza A (H1N1) vaccine virus was derived from a 2009 pandemic influenza A (H1N1) virus. Different formulations are recommended for the southern hemisphere, for example in 2017 this used a different influenza A H1N1 virus. A new high-dose trivalent inactivated vaccine is also available for use in those over 65 years of age but recent evidence suggests it may be just as cost effective to vaccinate more children, increasing herd immunity, as to vaccinate the elderly. Antibodies provide useful correlates of protection for most of these vaccines When antibodies provide protection, it is usually possible to determine a quantitative cut-off that is associated with protection. Seasonal influenza vaccines contain three flu strains, two A strains and one B strain. Antibodies to these strains induced by vaccination will protect against infection, but mutations in the influenza genes can cause antigenic drift leading to infection. When induced, protective immunity lasts for 1015 years and in one study lasted for over 50 years. In children over 6 years of age, or in those known or likely to have been infected with M. This vaccine was protective, but required very careful purification and inactivation to ensure it was safe, and was expensive to produce. The virus is grown in human cells, purified, inactivated with formaldehyde and adsorbed onto alum. Combined vaccines for hepatitis A and B are also available but as yet there is no vaccine available for hepatitis C. Some serological tests that provide correlates of protection for vaccines in current use are listed. Vaccines that are required for entry into particular countries, or for particular regions the yellow fever vaccine is required for entry into certain countries. A vaccination certificate may be required for all those entering a particular country, or for individuals coming from a country where yellow fever is endemic. Luckily this is a very immunogenic vaccine and a vaccination certificate is now valid for the life of the person vaccinated. A live attenuated (recombinant) tetravalent dengue vaccine is now licensed in some countries, having shown 79% protection against severe dengue in two phase 3 trials; this contains yellow fever viruses expressing surface membrane and pre-envelope proteins for the four dengue serotypes, with further vaccine candidates in development. However, it is important that the vaccine does not predispose the vaccinees to developing the severe forms of dengue haemorrhagic fever that can occur when someone is re-infected with dengue (see Ch. Finally, two inactivated viral vaccines for tick-borne encephalitis have been developed and are available in some countries.
Zofran Dosage and Price
Zofran 8mg
- 30 pills - $28.07
- 60 pills - $44.51
- 90 pills - $60.94
- 120 pills - $77.38
- 180 pills - $110.24
- 270 pills - $159.55
- 360 pills - $208.85
Zofran 4mg
- 60 pills - $28.76
- 90 pills - $35.55
- 120 pills - $42.34
- 180 pills - $55.92
- 270 pills - $76.28
- 360 pills - $96.65
Anteroposterior (A/P) projection: the x-rays travel from an anterior position medicine to reduce swelling order zofran american express, through the patient to reach the x-ray film/ detector that is posterior to the patient. Posteroanterior (P/A) projection: the x-rays travel from a posterior position, through the patient to reach the film/detector that is anterior to the patient. Lateral projection: the x-ray travels from one side, through the patient to reach the film/detector on the contralateral side. View: the most common descriptor noted in the text, view provides information about plane and axis orientation. Lateral view: A lateral view describes the image as if the viewer is looking at the image from the side, rather than from the front. Therefore, the left side of the image corresponds to the right side of the patient. Vertebrae are separated by fibrocartilaginous intervertebral discs and united through a series of joint, igaments, and capsules. Functionally, the vertebral column serves to protect the spinal cord and spinal nerves and support body weight superior to the pelvis. It also allows for varying degrees of m0tion arnsi plays an integral part in posture and gait. Most spinal motion occurs superior to the sacral level and is further dictated by articular orientation and bony attachments. Spinal motion includes extension, flexion, lateral side-bending, rotation, and circumduction. It most often occurs in the cervical region, although it can also be seen in the thoracic and lumbar regions. The etiology is not well defined, although patient age is a strong element in the development of spondylosis, which most often affects the geriatric patient population. Vertebral discs and facet joints are most vulnerable to degenerative changes, leading to narrowing of disc space/weakening of annulus fibrosis, and bone spur formation, respectively. Degenerative changes can also affect the adjacent posterior longitudinal ligament, which increases the risk of spinal cord compression as a result of disc herniation. Neurological symptoms-motor and sensory-associated with myelopathy and radiculopahty commonly drive patients to seek medical attention. Lumbosacral plain film radiograph revealing narrowing of disc space at the L3/L4 level (*). Vertebrae A vertebra is generally arranged as a weight-bearing body anteriorly, a vertebral (neural) arch and spinous process posteriorly, and transverse processes laterally. Vertebral body: the vertebral body is the weight-bearing portion of the vertebra and also serves as the site for intervertebral disc attachment. Vertebral arch: the vertebral arch protects the spinal cord and is formed by two pedicles that project posteriorly from the body and two laminae that meet in the mid line at the spinous process. Vertebral foramen: the vertebral canal houses the spinal cord and is formed by the collection of vertebral foramen along the length of the spine. Right and left sets of superior and inferior articular processes project from the junction of the pedicles and laminae. This procedure is performed to create more space in the vertebral canal, thus relieving pressure on the spinal cord and spinal nerve roots. Pressure is often caused by spinal stenosis (narrowing of the canal) as a result of a space-occupying lesion, such as excess bony growth, tumor formation, or disc herniation. Vertebral notches: Laterally, superior and inferior vertebral notches present as indentations posterior to the vertebral body. Spinal nerves and vasculature travel through intervertebral foramina on each side of the column. Sacral foramina: In the sacral region, spinal nerves exit the canal through anterior and posterior sacral foramina. Transverse processes in the thoracic region also articulate with ribs posteriorly and support the thoracic cage. Regional characteristics Regionally, vertebrae have distinct structural characteristics that further dictate function. For example, articular processes are oriented in different planes to allow or limit spinal mobility. Variations in size and shape can also allow for transmission of neural structures, such as the cervical and lumbar spinal cord enlargements, in respective regions. A foramen transversarium in the transverse processes accommodates vertebral vessels and sympathetic plexuses. It articulates with occipital condyles through two lateral masses (atlanto-occipital joint) and has a small anterior facet for articulation with the dens (odontoid process) of C2. C2 (axis): this vertebra is strong, featuring a dens that projects superiorly to articulate with C1 (pivot joint). C7 (vertebra prominens): this vertebra with its long, prominent spinous process makes a reliable surface landmark. In T1-T10 vertebrae, transverse processes have costal facets for articulation with rib tubercles, articular processes oriented in the frontal (coronal) plane, and long posteroinferiorly sloping, overlapping spinous process. Their articular facets are oriented in the sagittal plane, and they have short, hatched-shaped spinous processes. Facet orientation in the lumbar region is in the sagittal plane, which permits mainly flexion/extension and minimal rotation. Sacral (S1-S5): this fused, wedge-shaped bone is concave anteriorly and convex posteriorly. Pure dislocation in the thoracic and lumbar regions is less common and occurs in conjunction with additional factors, such as fracture, pathology, or congenital malformation. Some examples of dislocations with fractures are: · Spondylolysis (Scottie dog fracture): this stress fracture of the pars interarticularis is most commonly observed in young athletes at the L4 or L5 level. B, Plain film showing anterior position of L5 on sacrum, indicated by the yellow arrow.
© 2025 Adrive Pharma, All Rights Reserved..