General Information about Viagra Professional
Moreover, the extra-strength method of Viagra Professional is designed to supply a more constant and reliable response. This means that males taking Viagra Professional can expertise improved sexual performance and satisfaction with each use.
Viagra Professional is out there within the form of oral tablets and should be taken as prescribed by a health care provider. It should not be taken greater than once a day and should not be used with certain drugs or medical situations. It is crucial to tell a physician about any pre-existing medical conditions or drugs being taken earlier than starting therapy with Viagra Professional.
It is important to note that like all medication, Viagra Professional might cause unwanted side effects. These unwanted effects are usually mild and temporary, and will include headache, dizziness, facial flushing, or upset abdomen. However, if symptoms persist or become severe, it is important to seek the guidance of a healthcare professional.
One of the main benefits of Viagra Professional is its sooner onset of motion. While regular Viagra could take up to an hour to begin working, Viagra Professional can begin working in as little as 20 minutes. This is as a result of the higher focus of sildenafil citrate in Viagra Professional will increase the speed at which the drug is absorbed into the bloodstream.
Viagra Professional is a extremely efficient prescription drugs that has helped millions of males all over the world with erectile dysfunction (ED). Also often recognized as sildenafil citrate, this drug is a well-known and widely used treatment for ED. However, Viagra Professional takes the effectiveness of the long-lasting blue capsule to the next level.
Another benefit of Viagra Professional is its longer period of action. While common Viagra can last up to 4 hours, the consequences of Viagra Professional can last up to six hours. This makes it a more handy possibility for those trying to interact in sexual activity multiple instances within a short interval.
Like regular Viagra, Viagra Professional works by growing blood flow to the penis, which helps in reaching and sustaining an erection throughout sexual stimulation. However, the upper focus of sildenafil citrate in Viagra Professional allows for a stronger and longer-lasting erection, giving men the boldness and talent to perform better in the bedroom.
As an extra-strength model of Viagra, Viagra Professional is designed to supply quicker and longer-lasting outcomes. One of the key variations between common Viagra and Viagra Professional is the concentration of the lively ingredient, sildenafil citrate. While common Viagra incorporates 50mg or 100mg of sildenafil citrate, Viagra Professional contains 100mg, making it stronger and effective.
In conclusion, Viagra Professional is an extra-strength version of the well-known ED medicine, Viagra. With the next focus of the energetic ingredient, sildenafil citrate, it provides sooner onset of action, longer period of results, and a more consistent response. It is a highly efficient option for males seeking a more potent and dependable treatment for ED. However, it is important to seek the assistance of a physician and comply with the prescribed dosage and usage directions to make sure safe and efficient outcomes.
Antibody array characterization of inflammatory mediators in allergic and normal tears in the open and closed eye environments erectile dysfunction depression 100 mg viagra professional buy fast delivery. Membrane array characterization of 80 chemokines, cytokines, and growth factors in open- and closed-eye tears: angiogenin and other defense system constituents. Lymphocytic subpopulations in the normal human conjunctiva: a monoclonal antibody study. Changes in the concentration of secretory immunoglobulin A in tears during postoperative inflammation of the eye. Effects of castration and sex hormone administration on experimental allergic conjunctivitis. Differential distribution of neuronal markers and neuropeptides in the human lacrimal gland. Biological variation of immunoglobulin concentrations in normal human tears related to age and sex. Local antibody formation within the eye: a study of immunoglobulin class and antibody specificity. Effects of T-lymphocytedependent and -independent immunity on cholinergic enzyme activity in mouse lacrimal glands. Neuropeptides as signal molecules in common with leukocytes and the hypothalamic-pituitary-adrenal axis. Interferon-gamma enhances expression of secretory component, the epithelial receptor for polymeric immunoglobulins. The pathology of dry eye: the interaction between the ocular surface and lacrimal glands. Neural regulation of innate immunity: a coordinated nonspecific host response to pathogens. Experimental induction and three-dimensional two-photon imaging of conjunctiva-associated lymphoid tissue. Conjunctiva-associated lymphoid tissue current knowledge, animal models and experimental prospects. Neural-immune interrelationship: effect of optic, sympathetic, temporofacial, or sensory denervation on the secretory immune system of the lacrimal gland. Severe protein malnutrition: impact on tear IgA levels during development and aging. Influence of ocular surface antigen on the postnatal accumulation of immunoglobulin-containing cells in the rat lacrimal gland. Influence of gender, sex steroid hormones, and the hypothalamic-pituitary axis on the structure and function of the lacrimal gland. Do sex steroids exert sex-specific and/or opposite effects on gene expression in lacrimal and meibomian glands Composition and biophysical properties of the tear film: knowledge and uncertainty. Mucosal antibody response of calves after oral and intrabronchial administration of rotavirus. Diffusion of immunoglobulin G from the vascular compartment into the normal rabbit cornea. The concentration of lysozyme and secretory IgA in tears from healthy persons with and without contact lens use. Leu enkephalin-like immunoreactivity and the innervation of the rat exorbital gland. Effect of age, malnutrition and renutrition on free secretory component and IgA in secretions. Measurement of cytokines in the lacrimal gland and tears: analysis of various methods. The immunoarchitecture of the normal human lacrimal gland: relevancy for understanding pathologic conditions. Innervation and mast cells of the rat exorbital lacrimal gland: the effects of age. Sex hormone, glucocorticoid, and cytokine regulation of mucosal immunity: hormonal influences on antibody levels and antigen presentation in the female genital tract. Neural-immune interactions: an integrative view of the bidirectional relationship between the brain and immune systems. Distinct populations of dendritic cells in the normal human donor corneal epithelium. Immunohistochemical studies on whole mounts of the cornea and iris-ciliary body after corneal transplantation. Cholinergic stimulation of lactoferrin and epidermal growth factor secretion by the human lacrimal gland. Desiccating stress promotion of Th17 differentiation by ocular surface tissues through a dendritic cell-mediated pathway. The nasal cavity and the paranasal sinuses are bony chambers covered by a mucosal layer; different from the lower airways, these borders are fixed. Every sinus has got its own ostium through which it drains the mucus to the nasal cavity. The maxillary, frontal, and anterior ethmoidal sinuses drain in the middle meatus, underneath the middle turbinate. The sphenoidal and posterior ethmoidal sinuses drain in the superior meatus, underneath the superior turbinate. This mucosal layer is covered by a mucus blanket in which microbes, dust, and irritant particles are easily trapped.
Natural antibodies can neutralize influenza virus (Choi and Baumgarth erectile dysfunction pump canada trusted 50 mg viagra professional, 2008) via two possible mechanisms: either transport to the mucosal the Mucosal Immune Response to Respiratory Viruses Chapter 94 1807 antibody-dependent cellular cytotoxicity (Hashimoto et al. It is currently unknown if lung immune cells rely solely on these helicases to recognize particular viral infections or certain phases of the replicating virus. In viral infection, the endoplasmic reticulum, the cellular protein secretion machinery of the cell, is often hijacked to the benefit of the virus. However, the ensuing inflammation can exacerbate disease severity and can cause death from acute lung injury (Lin et al. This implies that an unbalanced immune response can have detrimental effects on systemic illness and survival. This cytokine production also contributes to lung pathology and may not be essential for virus clearance because viral clearance is not affected when costimulatory signals are blocked (Hufford et al. Excess T cell infiltration into the virally infected lung compromises lung function and compliance. The molecular mechanisms of how this occurs have been the subject of intense research (reviewed in Neyt et al. Leukocyte compartments in the mouse lung: distinguishing between marginated, interstitial, and alveolar cells in response to injury. B-1 and B-2 cell-derived immunoglobulin M antibodies are nonredundant components of the protective response to influenza virus infection. Surfactant protein A modulates the differentiation of murine bone marrow-derived dendritic cells. Surfactant protein D enhances bacterial antigen presentation by bone marrow-derived dendritic cells. Induction of high-affinity IgE receptor on lung dendritic cells during viral infection leads to mucous cell metaplasia. From skin dendritic cells to a simplified classification of human and mouse dendritic cell subsets. House dust mite allergen induces asthma via Toll-like receptor 4 triggering of airway structural cells. Antibody-dependent cellmediated cytotoxicity against influenza virus-infected cells. Dendritic cell subsets in primary and secondary T cell responses at body surfaces. Natural antibody and complement mediate neutralization of influenza virus in the absence of prior immunity. Cross-reactive influenza-specific antibody-dependent cellular cytotoxicity antibodies in the absence of neutralizing antibodies. Plasmacytoid dendritic cells induce plasma cell differentiation through type I interferon and interleukin 6. Differential type I interferon induction by respiratory syncytial virus and influenza a virus in vivo. An unbiased analysis of V(H)-D-J(H) sequences from B-1a, B-1b, and conventional B cells. Selective rejection of H-2-deficient lymphoma variants suggests alternative immune defence strategy. Interleukin-18 improves the early defence system against influenza virus infection by augmenting natural killer cell-mediated cytotoxicity. Innate lymphoid cells promote lung-tissue homeostasis after infection with influenza virus. T cell- and B cell-independent adaptive immunity mediated by natural killer cells. Control of early viral and bacterial distribution and disease by natural antibodies. Airway epithelial cells regulate the functional phenotype of locally differentiating dendritic cells: implications for the pathogenesis of infectious and allergic airway disease. MyD88-mediated instructive signals in dendritic cells regulate pulmonary immune responses during respiratory virus infection. Mice can recover from pulmonary influenza virus infection in the absence of class I-restricted cytotoxic T cells. Alveolar macrophages are essential for protection from respiratory failure and associated morbidity following influenza virus infection. Natural killer cells in mouse lung: surface phenotype, target preference, and response to local influenza virus infection. Plasmacytoid dendritic cells are dispensable during primary influenza virus infection. Identification of a novel antigen-presenting cell population modulating antiinfluenza type 2 immunity. The mechanisms leading to the prominent predilection for the lungs are of major interest. Protracted cavitary disease of the lungs is mandatory for the transmission of aerosol infection to susceptible subjects within the population. This advantage for the pathogen could have influenced the evolution of those structural constituents of tubercle bacilli, which determine the predilection for the lungs. In this poorly acidified environment, bacilli are protected from being killed while recruiting nutrients for replication. Egress of Mtb into the cytosol has been demonstrated in vitro, but doubts have been expressed as to whether it occurs in vivo, hence this subject remains a matter of ongoing controversy (Harriff et al. Although the lungs appear to be the "locus minoris" for entry and infection, humans evolved potent resistance mechanisms, which restrain Mtb organisms in a latent form and prevent the development of active disease in over 90% of infected subjects with an unimpaired immune system. This protection develops during adolescence, involving multiple genetic factors and both innate and acquired immunity. Predilection of Mtb infection in the lungs is apparent from the finding that respiratory inoculation of smaller doses of Mtb causes more severe pathology and mortality than much larger doses given systemically (North, 1995).
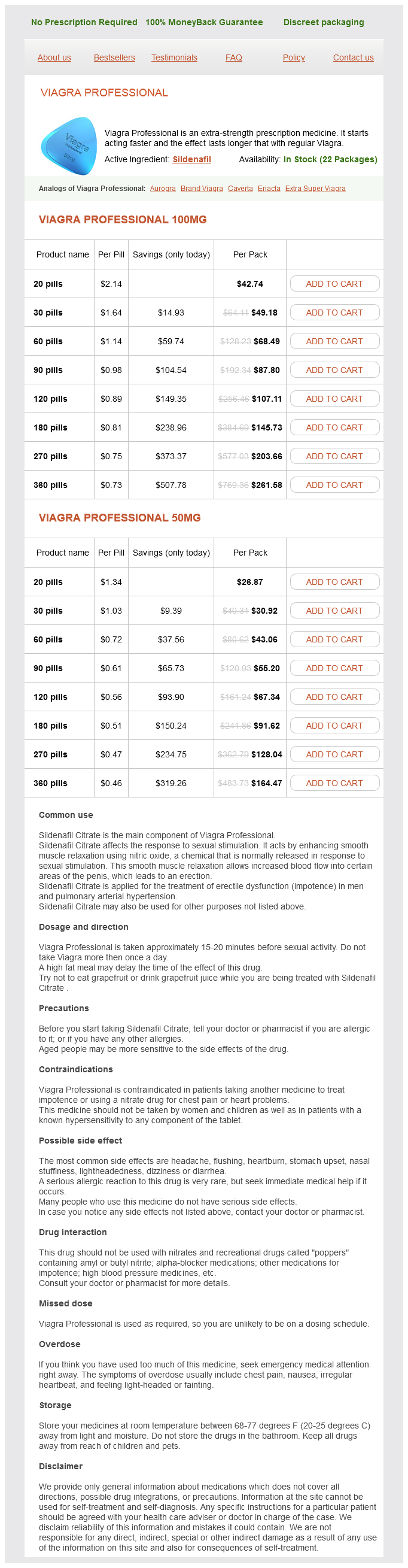
Viagra Professional Dosage and Price
Viagra Professional 100mg
- 20 pills - $42.74
- 30 pills - $49.18
- 60 pills - $68.49
- 90 pills - $87.80
- 120 pills - $107.11
- 180 pills - $145.73
- 270 pills - $203.66
- 360 pills - $261.58
Viagra Professional 50mg
- 20 pills - $26.87
- 30 pills - $30.92
- 60 pills - $43.06
- 90 pills - $55.20
- 120 pills - $67.34
- 180 pills - $91.62
- 270 pills - $128.04
- 360 pills - $164.47
Clinically erectile dysfunction treatment herbal remedy safe 50 mg viagra professional, this was accompanied by poor weight gain, diarrhea, and occult blood loss. Epithelial cells in the deficient mice were flatter and exhibited increased proliferation compared with those in normal mice, whereas goblet cells had a shrunken appearance. As expected, Muc2 could not be detected in the reduced mucin layer, but another mucin, Muc6, was detected along with trefoil factor-3. Overall, these studies clearly defined Muc2 deficiency and loss of epithelial barrier function resulting from such a deficiency as a cause of colonic inflammation. In another model of colitis resulting from a mucus abnormality, a particular O-glycan component of the Muc2, core3-derived O-glycan, was the focus of study (An et al. Mice with such a deficiency exhibit increased epithelial permeability but no evidence of trans-epithelial passage of bacteria. In addition, they exhibit increased proinflammatory cytokine production including increased production of Th1 and Th17 cytokines. In a related model, mice with deficiency of core 1-derived O-glycan were the focus of study (Fu et al. Deletion of core 1-derived O-glycan was accomplished by conditional deletion of a floxed gene expressing this enzyme along with Cre-recombinase expressing only epithelial cells so that deletion of the gene was limited to the latter cells. Young mice with such a deletion promptly developed colitis that was particularly severe in the distal colon and rectum and was characterized by epithelial ulceration, crypt microabscess formation, and thickened intestinal walls. Not surprisingly, deficient mice exhibited a reduced inner mucous layer and Muc2 expression, along with increased intestinal permeability to both proteins and bacteria. In a final series of studies relating to mice with core 1 O-glycan deficiency, such a deficiency was associated with expression of the Tn antigen, i. Overall, these models of intestinal inflammation relating to Muc2 abnormalities provide incontrovertible evidence that Muc2 deficiency or, perhaps more important, Oglycan abnormalities leading to Muc2 deficiency, can cause colitis. P-gp is a transmembrane glycoprotein whose function is necessary for normal epithelial barrier function. In addition, P-gp deficiency leads to increased translocation of bacteria into the lamina propria and the disease is ameliorated by antibiotic treatment (Resta-Lenert et al. It is therefore apparent that colitis in these mice arises, at least in part, from a barrier defect causing excessive penetration of microbiome organisms or products that is similar in its effect, if not in its cause, to that leading to colitis in mucus protein abnormalities. Pyroptosis normally occurs in myeloid cells when the latter are invaded by pathogenic organisms and is an innate response to infection. One possibility is that P-gp has an unexpected role in myeloid cells that protects the latter from untoward Ulcerative Colitis Chapter 81 1595 inflammatory responses possibly induced by commensal organisms. In initial studies it was observed that a single dose of intrarectal oxazolone elicits inflammation of the distal half of the colon characterized by intense infiltration of the mucosal layer composed of mononuclear cells admixed with a lesser population of polynuclear cells (Boirivant et al. This inflammation rapidly intensifies and in doing so causes obliteration of villous architecture, significant bowel wall edema, micro-ulcerations, and luminal exudates. Typically, the inflammation thus elicited evolves over 34 days, after which the mouse either succumbs or recovers. However, if mice are presensitized with subcutaneous oxazolone before intra-rectal challenge with oxazolone, a more chronic lesion with characteristics similar to the acute lesion ensues that lasts on the order of 12 weeks (Heller et al. This anti-inflammatory feature of the inflammation may be responsible for the short duration of disease as well as its limitation to the distal colon. Epithelial cell damage resulting from these mechanisms of cell injury would account for the development of epithelial ulcerations and breaks in oxazolone colitis and could also lead to entry of commensal bacteria into the lamina propria that would also induce an inflammatory effect. As such, it provides a powerful tool with which to design studies of its human counterpart. However, such ulcerative lesions can have secondary effects that also contribute to the inflammation deeper in the intestinal wall. Finally, epithelial ulceration resulting from these processes allows entry of bacterial components into the lamina propria that stimulates secondary inflammatory reactions. Because of the Th2 orientation of the disease, it is not surprising that these cytokines are among those that augment Th2 responses. In some cases this facilitates pathogenic responses in mucosal tissues including epithelial cell hyperplasia and enhanced recruitment of inflammatory cells into inflamed areas. However, a report indicated that bioactive mature forms not dependent on caspase cleavage may be generated (Lefrancais et al. Such entry, as noted above, is itself a cause of inflammation regardless of the original mechanism of colitis. This possibility does not posit the presence of an altered microbiome as the initiator of the stress response because it appears equally likely that the stress response could arise from interactions between epithelial cells and normal microbiome constituents. This view is based on the fact that most changes observed in experimental models of barrier defects lead to enhanced inflammation caused by a more primary immunologic response and in Ulcerative Colitis Chapter 81 1601 those instances in which the barrier defect per se leads to gut inflammation. Its uniqueness begins with its strict intestinal confinement to the colon, which points at once to the likelihood that the disease is triggered and maintained by the rich microbiome that populates this site. This fits with the hypothesis that an epithelial cell defect (perhaps of several types) initiates the disease under pressure from the colonic microbiome. Finally, and perhaps most important, the uniqueness of this disease lies in the distinct type of pathogenic immunologic process associated with and driving the inflammation. Hepatocyte nuclear factor 4alpha in the intestinal epithelial cells protects against inflammatory bowel disease. Inflammatory bowel disease in the AsiaPacific area: a comparison with developed countries and regional differences. Regulation of mucosal structure and barrier function in rat colon exposed to tumor necrosis factor alpha and interferon gamma in vitro: a novel model for studying the pathomechanisms of inflammatory bowel disease cytokines.
© 2025 Adrive Pharma, All Rights Reserved..