General Information about Valsartan
The typical dosage of valsartan is between 80-160 milligrams per day, taken orally. It is normally taken as quickly as a day, with or with out meals. It is important to take this treatment as prescribed by a healthcare professional, and to not modify the dosage or stop taking it with out consulting a well being care provider. It could take a few weeks for valsartan to succeed in its full effectiveness, so it is important to continue taking it even if there isn't a instant change in blood stress.
Besides treating high blood pressure, valsartan is also used to prevent coronary heart failure and to enhance survival rates after a heart assault. It has additionally been discovered to be effective in preventing kidney damage in folks with kind 2 diabetes.
Valsartan belongs to a gaggle of medicines generally recognized as ARBs, which work by blocking the motion of angiotensin II, a hormone that causes blood vessels to narrow and blood strain to extend. By blocking the consequences of this hormone, valsartan helps to dilate or widen the blood vessels, allowing for improved blood circulate and decreased blood stress.
Valsartan is contraindicated in pregnant ladies, as it could hurt the growing fetus. It can be not really helpful for individuals who have a history of angioedema, a condition characterized by swelling of the face, lips, tongue, or throat.
High blood strain is a critical well being condition that affects hundreds of thousands of people worldwide. It can result in various issues such as coronary heart illness, stroke, and kidney failure. It is commonly referred to as the 'silent killer' as a outcome of it normally doesn't trigger any signs till it has caused important damage to the body.
Valsartan, also identified by its brand name Diovan, is a generally prescribed medicine used to treat hypertension, also called hypertension. It is classified as an angiotensin receptor blocker (ARB) and works by enjoyable the blood vessels, allowing for higher blood circulate and lowering blood strain.
Valsartan can also work together with other drugs, together with nonsteroidal anti-inflammatory medicine (NSAIDs), certain antibiotics, and potassium supplements. It is crucial to tell a healthcare professional about all medicines, dietary supplements, and herbs being taken before beginning valsartan to avoid any potential interactions.
Like any treatment, valsartan may cause unwanted effects, though not everyone will experience them. Common side effects could embody dizziness, headaches, and nausea. In some instances, extra severe unwanted effects could happen, together with allergic reactions, liver issues, and low blood strain. It is essential to seek medical consideration if any of these symptoms occur.
In summary, valsartan is a extensively prescribed ARB that has been proven to be an efficient and secure therapy for high blood pressure. It works by enjoyable blood vessels, improving blood circulate, and reducing blood stress. As with any medicine, it is very important comply with the prescribed dosage and inform a healthcare skilled of any existing medical circumstances or drugs being taken. With proper use and monitoring, valsartan can successfully help manage and management hypertension, leading to raised general well being and a decreased risk of complications.
The prognosis for any disease may be influenced by medical or surgical intervention; indeed that is the objective blood pressure joint pain valsartan 40 mg order without prescription. So one must distinguish between the prognosis for a disease that is allowed to follow its natural course and the prognosis for the same disease in a group of patients receiving appropriate therapy. In assessing the long-term prognosis for a chronic disease, it is important to compare the survival of a group of patients with actuarial data for comparable populations without the disease. The survival data for the group with the disease should be corrected to allow for deaths that are likely to occur from other diseases. Some are punctuated by periods of quiescence when the patient enjoys relatively good health. Some diseases may oscillate through several cycles of remission and relapse before the patient is cured of or succumbs to the disease. The tendency of some diseases to go through cycles of remission and relapse can make it difficult to be certain about prognosis in an individual case. For example, a non-fatal myocardial infarct (heart attack) leaves an area of scarring of the myocardium, impairing its contractility and predisposing to heart failure: this is the morbidity of the disease in that particular patient. Mortality is expressed usually as a percentage of all those patients presenting with the disease. For example, the mortality rate of myocardial infarction could be stated as 50% in defined circumstances. Until the 19th century, many diseases and causes of death were recorded in a narrative form, often based on symptoms. The early medical statisticians, William Farr (18071883) and Jacques Bertillon (18511922), pioneered a systematic and uniform approach to disease classification, thereby laying the foundations of modern disease nomenclature. Primaryandsecondary the words primary and secondary are used in two different ways in the nomenclature of disease: 1. Primary in this context means that the disease is without evident antecedent cause. Other words with the same meaning are essential, idiopathic, spontaneous and cryptogenic. Thus, primary hypertension is defined as abnormally high blood pressure without apparent cause. Secondary means that the disease represents a complication or manifestation of some underlying lesion. Thus, secondary hypertension is defined as abnormally high blood pressure as a consequence of some other lesion. The words primary and secondary may be used to distinguish between the initial and subsequent stages of a disease, most commonly in cancer. The primary tumour is the initial tumour from which cancer cells disseminate to cause secondary tumours elsewhere in the body. Disabilityanddisease Many diseases result in only transient disability; for example, influenza or a bad cold may necessitate time off work for an employed person. Some diseases, however, are associated with a significant risk of permanent disability; in such cases, treatment is intended to minimise the risk of disability. Some investigations and treatments carry a small risk of harm, often permanent, and the risk of disability must be outweighed by the potential benefit to the patient. Generally, the earlier a disease is diagnosed, the smaller the risk of disability either from the disease itself or from its treatment. This is one of the main objectives of screening programmes for various conditions. The objective assessment, preferably measurement, of disability is important in the evaluation of the impact of a disease or the adverse effects of its treatment. There is, for example, a balance between the longevity of survival from a disease and the quality of life during the period of survival after diagnosis: a treatment that prolongs life may be unacceptable because it prolongs suffering; treatment that makes a patient more comfortable, but does not prolong life and may actually shorten it, may be more acceptable. Acuteandchronic Acute and chronic are terms used to describe the dynamics of a disease. Acute conditions have rapid onset, often but not always followed by rapid resolution. Chronic conditions may follow an acute initial episode, but often are of insidious onset, and have a prolonged course lasting months or years. Thus, benign tumours remain localised to the tissue of origin and are very rarely fatal unless they compress some vital structure. Benign hypertension is relatively mild elevation of blood pressure that develops gradually and causes insidious injury to the organs of the body. Suffixes Commonly used suffixes and their usual meanings are: resulting in obesity, hirsutism, hypertension, etc. Numericaldiseasecodingsystems Standard numerical codes, rather than names, are often used for disease registration and in epidemiological studies. Eponymous names are used commonly either when the nature or cause of the disease or lesion is unknown, or when long-term usage has resulted in the name entering the language of medicine, or to commemorate the person who first described the condition. Disease classifications are creations of medical science and are justified only by their utility. Classifications are useful in diagnosis to enable a name (disease or disease category) to be assigned to a particular illness. Disease classification at a relatively coarse level of categorisation is unlikely to change quickly. However, the more detailed the level of classification, the more likely it is to change as medical science progresses. The general classification of disease into categories such as inflammatory and neoplastic (see below) is long established. Most diseases can be assigned a place in the following classification: · congenital · Syndromes - genetic (inherited or sporadic mutations) - non-genetic acquired - inflammatory - haemodynamic - growth disorders - injury and disordered repair - disordered immunity - metabolic and degenerative disorders. First, the above classification is not the only possible classification of disease.
Ferritin is present in all tissues blood pressure medication cause weight gain purchase valsartan 80 mg amex, but especially in the macrophages of the bone marrow and spleen and in hepatocytes. A small amount is detectable in plasma and, as it is derived from the storage pool of body iron, its concentration is thus an accurate indicator of body iron stores. Low serum ferritin concentration is a useful confirmatory test for iron deficiency. However, because ferritin is an acute-phase response protein, the concentration in plasma is not a reliable guide to body iron stores in the presence of infection, inflammation and neoplasia. Ferritin is water soluble and not visible by light microscopy; haemosiderin is insoluble and forms yellow granules. When iron stores are normal, haemosiderin is visible, mainly in the reticuloendothelial cells of the bone marrow. In iron overload, most of the iron is in the form of haemosiderin and can easily be identified. Transferrin is an iron-binding beta-globulin responsible for iron transport and delivery to receptors on immature erythroid cells. Each molecule of transferrin can bind two atoms of iron, but normally the transferrin is only onethird saturated (thus the serum iron concentration is normally one-third of the total serum iron-binding capacity) providing readily available excess capacity to increase iron transport from the gut, if needed. A low transferrin saturation is therefore diagnostic of iron deficiency while high levels are a feature of iron overload with deposition of iron in tissues. In order to maintain iron balance, sufficient iron must be absorbed to replace that lost from the urinary and gastrointestinal tracts as shed cells and in sweat, together with any extra requirements. Daily iron requirements are: · · · · adult male child pregnant female menstruating female 1. Thus, loss of 10 mL of blood daily will inevitably exceed the capacity to absorb sufficient iron, even from a good diet. This explains the finding of some degree of iron depletion in 25% or more of menstruating women. Haem iron is present in meat and is readily absorbed, with little effect from other dietary components. Inorganic iron in vegetables and cereals is mostly trivalent and may be complexed to amino acids and organic acids, from which it must be released and reduced to the divalent state for absorption. In contrast, phosphates and phytates in some foods form precipitates and prevent absorption. Mechanisms controlling the rate of iron absorption are becoming better understood. Hepcidin binds to ferroportin and internalises it, trapping iron within iron-exporting cells. Iron loading leads to rapid production of hepcidin by the liver which, in turn, inhibits intestinal iron absorption and movement of iron from stores. This is achieved by hepcidin down-regulating the plasma membrane transfer protein ferroportin. Iron is consequently trapped in iron-exporting cells, including duodenal enterocytes. Mechanisms of iron deficiency In developed countries, iron deficiency in the nonmenstruating and non-pregnant adult most frequently results from chronic blood loss, often from the gastrointestinal tract. As it is possible to lose several millilitres of blood daily into the gut lumen without marked change in appearance of the stool, such blood loss is frequently occult. Iron deficiency anaemia is thus commonly a presenting feature of lesions within the gastrointestinal tract. In clinical practice, when iron deficiency anaemia occurs in the face of a reasonable diet and no excessive menstrual loss, it is mandatory to perform a careful assessment of the gastrointestinal tract. There is central pallor of the erythrocytes and poikilocytosis with elongated (pencil or cigar) cells. The microcyte results from an extra cell division, in addition to the normal four, during red cell production. Increasing cytoplasmic haemoglobin concentration normally acts as an inhibitor of normoblast division. The failure of haemoglobin synthesis that results from iron deficiency therefore allows extra mitoses to occur, with the production of small erythrocytes. The same mechanism is responsible for the microcytes in thalassaemia, another disorder of haemoglobin synthesis. The proportion of polychromatic cells (or reticulocytes) is low for the degree of anaemia, indicating an inability of the bone marrow to respond due to lack of iron for haemoglobin synthesis. Changes in other organs and tissues In addition to the manifestations of chronic anaemia, a variety of epithelial changes may be present in chronic iron deficiency: 572 is often raised, especially if chronic bleeding is present. Occasionally, a mixture of microcytic, hypochromic erythrocytes and macrocytic cells is seen. This is termed a dimorphic picture and occurs in mixed deficiency of iron and folic acid or vitamin B12. In the former circumstance, mildly increased polychromasia (and reticulocytosis) may be present. The nucleated red cell precursors are small in diameter and the cytoplasm is frequently ragged micronormoblastic erythropoiesis. Important biochemical changes in the blood are a fall in serum iron and increase in total iron-binding capacity (representing a compensatory increased transferrin concentration). Saturation of iron-binding capacity is thus reduced to 10% or less, from the normal 33%. The serum ferritin is generally markedly reduced, corresponding to severely depleted body iron content.
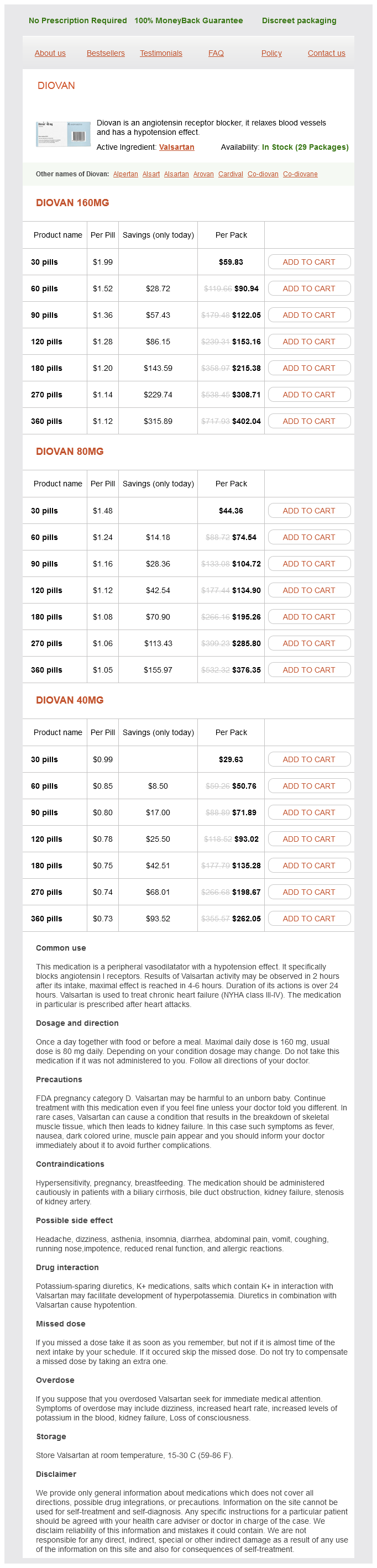
Valsartan Dosage and Price
Diovan 160mg
- 30 pills - $59.83
- 60 pills - $90.94
- 90 pills - $122.05
- 120 pills - $153.16
- 180 pills - $215.38
- 270 pills - $308.71
- 360 pills - $402.04
Diovan 80mg
- 30 pills - $44.36
- 60 pills - $74.54
- 90 pills - $104.72
- 120 pills - $134.90
- 180 pills - $195.26
- 270 pills - $285.80
- 360 pills - $376.35
Diovan 40mg
- 30 pills - $29.63
- 60 pills - $50.76
- 90 pills - $71.89
- 120 pills - $93.02
- 180 pills - $135.28
- 270 pills - $198.67
- 360 pills - $262.05
The microadenoma is a small neoplasm blood pressure medication lower testosterone discount valsartan 80 mg line, measuring less than 10 mm in diameter, with no mechanical effects and usually discovered only during intensive investigation of infertility; the lesion often produces prolactin in excess. Oxytocin Oxytocin is an aptly named hormone (it is the Greek word for quick birth) as it stimulates the uterine smooth muscle to contract. Interestingly, it is oxytocin from the fetal pituitary that plays the greater role in initiating parturition, suggesting that the fetus orders its own birth. The tumours are almost certainly of neuroendocrine origin and thus equipped for the synthesis of peptide hormones. Little is known of its function, although its secretory product, melatonin, is thought to be involved in circadian rhythm control and gonadal maturation. The most important tumours of the pineal gland are malignant germ cell tumours (teratomas and seminomas) and pinealoblastomas, resembling neuroblastomas. The medulla, of neural crest embryological origin, is part of the sympathetic nervous system; it secretes catecholamines, which are essential in the physiological responses to stress, The cortex, derived from mesoderm, synthesises a range of steroid hormones with generalised effects on metabolism, the immune system, and water and electrolyte balance. Islands of similar tissue, known as the organs of Zuckerkandl, are sometimes found in other retroperitoneal sites; these have similar functions and a similar pattern of diseases to that seen in the adrenal medulla. Catecholamines are secreted in states of stress and of hypovolaemic shock, when they are vital in the maintenance of blood pressure by causing vasoconstriction in the skin, gut and skeletal muscles. Other associations are with neurofibromatosis and the rare von HippelLindau syndrome. It is not generally possible to predict this behaviour from the histological appearance. Neuroblastoma Neuroblastoma is a rare and highly malignant tumour found in infants and children. The adrenal medulla is expanded by a dark-coloured tumour with areas of degeneration and haemorrhage. The tumour presents through the effects of its catecholamine secretions: hypertension (which is sometimes intermittent), pallor, headaches, sweating and nervousness. Although it is a rare cause of hypertension, phaeochromocytoma must not be overlooked as it is one of the few curable causes of elevated blood pressure; other causes include adrenal cortical adenoma, renal artery stenosis and aortic coarctation. There are groups of cells with granular cytoplasm, amidst which there are numerous branching capillaries. Neuroblastomas may also originate from parts of the sympathetic chain outside the adrenal medulla. Secondary spread to liver, skin and bones (especially those of the skull) is common. Surprisingly, neuroblastoma may occasionally mature spontaneously to ganglioneuroma, a benign tumour. The most important of the hormones is cortisol (hydrocortisone), but other steroid metabolites have similar effects. Mineralocorticoids the most important of the mineralocorticoids, aldosterone, acts on the renal tubules to increase reabsorption of sodium and chloride, reducing their loss in urine at the expense of potassium exchange. Steroid hormones Glucocorticoids the glucocorticoids have important effects on a wide range of tissues and organs. At physiological levels they: · inhibit protein synthesis · increase protein breakdown · increase gluconeogenesis. The normal zones are: zona glomerulosa (top), zona fasciculata (middle) and zona reticularis (bottom). However, virilising androgens may be produced in conditions such as certain congenital enzyme defects and adrenal cortical tumours, especially if these are malignant. Hyperfunction Hyperfunction of the adrenal cortex produces generalised effects, the nature of which depends on whether glucocorticoids, mineralocorticoids or sex steroids are produced in excess. The syndrome occurs most commonly in adult women, and sometimes there is also excess androgen production causing virilisation. Diagnosis Diagnosis is by demonstration of glucocorticoid excess, either as elevated plasma levels of cortisol or as elevated urinary excretion of 17-hydroxysteroids, degradation products of glucocorticoids. This was the cause of the syndrome originally described by Harvey Williams Cushing, a Boston neurosurgeon with an interest in the pituitary. Histologically, the cells of the adrenal cortex may appear depleted of lipid, indicating that they have discharged their secretions into the blood. Diagnosis the diagnosis of primary hyperaldosteronism rests on two criteria: plasma aldosterone must be raised while renin is low. This is to distinguish it from secondary hyperaldosteronism, in which aldosterone levels are raised but are an appropriate response to high renin levels. The usual cause is an adenoma of the zona glomerulosa, but generalised hyperplasia of the zona is sometimes responsible. The resulting renal retention of sodium and water leads to hypertension, while potassium loss leads to muscular weakness and cardiac arrhythmias. The hypokalaemia is associated with metabolic alkalosis, causing tetany and paraesthesiae. This physiological response is known as Hypersecretionofsexsteroids Some adrenal cortical adenomas secrete sex steroids, most commonly androgens. Rarely, congenital enzyme defects of the pathways of steroid synthesis may result in excess production of sex steroids. The resulting excess intermediate steroids are converted to androgens, leading to virilisation. A pale-coloured fleshy nodule in the adrenal cortex is displacing the medulla and stretching out the rest of the cortex.
© 2025 Adrive Pharma, All Rights Reserved..