General Information about Telmisartan
In summary, telmisartan, sold underneath the brand name Micardis, is an effective treatment for the remedy of high blood pressure and lowering the risk of heart assault and stroke. As with any treatment, it is essential to observe the physician's directions and to communicate any considerations or changes in well being standing. By taking Micardis as prescribed, individuals can successfully manage their blood stress and cut back the danger of harmful issues.
Micardis comes within the type of oral tablets, that are often taken once per day. The dosage could range depending on the patient's situation and other components, such as age, weight, and response to therapy. It is essential to take the treatment as prescribed and to not exceed the really helpful dose.
People with sure medical situations, such as kidney illness or liver disease, may require special monitoring whereas taking Micardis. Also, it's important to tell the physician of some other drugs being taken, as some medication might work together with telmisartan and affect its effectiveness or enhance the risk of unwanted effects.
Micardis works by blocking the angiotensin II receptors within the physique, which causes the blood vessels to chill out and widen, allowing for improved blood flow and decreased blood pressure. This mechanism of motion is different from different lessons of blood stress medication, such as beta blockers or diuretics, which work by slowing the center rate or lowering fluid within the body.
In addition to treating hypertension, telmisartan can additionally be prescribed for patients with a current history of heart attack or stroke. By decreasing blood pressure, this treatment can reduce the danger of future cardiovascular events.
Telmisartan, also recognized by its brand name Micardis, is a medication primarily used for the treatment of hypertension, or hypertension. It is classified as an angiotensin receptor blocker (ARB) and works by blocking the action of angiotensin II, a hormone that causes blood vessels to constrict and lift blood strain.
Hypertension is a standard and critical well being situation that affects hundreds of thousands of individuals worldwide. If left unmanaged, it could result in severe complications such as coronary heart disease, stroke, and kidney failure. Telmisartan is amongst the drugs prescribed by medical doctors to help management and handle high blood pressure.
Like all medicines, telmisartan might trigger unwanted effects in some individuals. Common side effects embody dizziness, fatigue, and headache. These side effects are normally delicate and resolve on their very own. However, in the occasion that they persist or become bothersome, you will want to communicate with a doctor.
Telmisartan is out there as both a standalone treatment and in combination with other drugs, similar to hydrochlorothiazide, to supply a quantity of modes of motion for blood pressure management. It is necessary to notice that Micardis is not a treatment for hypertension, but quite a tool for managing it. Therefore, it's crucial to proceed taking the treatment even when blood stress has stabilized to stop a sudden improve in readings.
Clinically arrhythmia in 7 year old purchase telmisartan now, it presents as chronic dysfunction of the lung allograft and is associated with a high mortality rate. Histologically, partial or complete obstruction of the bronchiolar lumina is seen. In case of complete obstruction, bronchioles can be recognized by their muscle layer, their elastic layer (elastic stain), or the accompanying pulmonary artery. Scattered alveolar epithelial cells exhibit enlarged nuclei with intranuclear inclusions. Discussion Cytomegalovirus infection remains a substantial issue for lung transplant recipients. Histologically, the most typical finding is chronic interstitial pneumonia with the characteristic cytopathic effect. In addition to histology, studies for clonality and Epstein-Barr virus play a role in the diagnosis. The slide is from a transbronchial biopsy performed during the bronchoscopy procedure. Pathologic Findings Histologic sections show foci of airspace-filling fibroblastic plugs. Discussion Organizing pneumonia is a relatively common finding in posttransplant lung biopsies. However, after lung transplantation, it may also be related to aspiration, infection, and acute rejection. Histologically, airspaces are focally filled with fibroblastic plugs (Masson bodies). Pathologic Findings the lung biopsy shows effaced pulmonary parenchyma with an infiltrate composed of large atypical lymphoid cells. Epstein-Barr virus in situ hybridization is positive with a diffuse staining pattern. Sometimes called dense core granules, these structures are round and characterized by an electron dense center surrounded by an outer membrane. As a result, their detection is most specific for the presence of these granules, but detection is dependent on the number of these granules within the tumor. Therefore, in addition to the number of granules present, the composition and balance between chromogranin A and B determines the sensitivity of this marker. In practice, some tumors will produce synaptophysin without detection of chromogranin, whereas others produce chromogranin without synaptophysin. However overall, synaptophysin is more sensitive than chromogranin and somewhat less specific. In one series, 27% of morphologically squamous carcinomas and adenocarcinomas were synaptophysin positive,10 a finding common to other series. Although the sensitivity of this marker is often highest among the commonly used neuroendocrine markers, nonneuroendocrine carcinomas may be positive for this protein, including ovarian stromal tumors, endometrial stromal sarcoma, synovial sarcoma, thyroid neoplasms, and natural killer cells. Neuron-specific enolase is an enzyme found in neurons and neuroendocrine cells, and for a time it was the only consistent marker of neuroendocrine differentiation. As a result, the most sensitive reagents will cross-react with many nonneuroendocrine tumors,14 and attempts to create more specific reagents have resulted in loss of sensitivity or technically difficult protocols. There has been movement toward uniformity of nomenclature for these tumors, especially within the gastrointestinal tract and pancreas. This has resulted in a grading schema that incorporates low-grade, intermediate-grade, and high-grade neuroendocrine tumors. The earliest investigations of scattered cells within secretory mucosa of the gastrointestinal tract had in common the recognition that there were cells within the mucosa oriented away from the lumen and identifiable through histochemical reactions with silver salts. These first observations raised issues as to the possibility of secretion into the vasculature rather than the luminal space, and also allowed for a method of detection in various organs. These cells were given different names including enterochromaffin, argentaffin, and Kulchitsky cells based on their staining characteristics and the histologist who studied them. Oberdorfer coined the term Karzinoid tumoren and Masson raised the possibility that these tumors were related to Kulchitsky cells with a secretory endocrine nature. Feyrter suggested that such cells were diffusely distributed among mucosal surfaces, and introduced a diffuse neuroendocrine system. However, experimental evidence mounted that these cells were not of neural crest origin, and further studies showed that thyroid C-cells, melanocytes, myenteric plexus, and paraganglia were of neural crest origin, but not the neuroendocrine cells of various mucosal linings. However, the relationship of these cells to both epithelia and neural structures is a critical functional interface, and the spectrum of differentiation within these cells shows their own ability to straddle epithelial and spindle/neural-like differentiation. These cells are thought to be important during lung embryogenesis and in fact are more plentiful in fetal lung. Although neuroendocrine tumors are immunoreactive, a subset of nonneuroendocrine tumors is also positive for this marker. Cushing syndrome has been rarely described in multiple carcinoid tumorlets;24 in some cases, multiple tumorlets are associated with a carcinoid tumor in these cases. Because it is found in association with tumorlets and carcinoids, this definition goes on to include these entities. Carcinoid tumorlets are nodular proliferation of neuroendocrine cells, usually with an invasive growth pattern through the airway wall, measuring 5. The definition becomes increasingly complicated in settings where the background chronic lung disease can lead to histologic neuroendocrine hyperplasia, but where multifocality cannot be assessed or when imaging or clinical manifestations are not present. An airway-based process may be associated with thickening of bronchial and bronchiolar walls and airway dilatation may also be present. In areas of airway constriction, hypoxic vasoconstriction results in decreased perfusion and lower attenuation. The presence of nodules varies by study, but in one retrospective series based on pathologic diagnosis, nodules were found in all cases.
Rare cases may be associated with demyelination showing rare or even no tumor cells39; this rare complication tends to occur several years after initial presentation hypertension unspecified buy telmisartan 40 mg fast delivery. Although ultrastructural demonstration of Birbeck granules was of great historical relevance in the definition of this tumor type, electron microscopy is rarely performed today. Those involving the dura may mimic meningioma, whereas those involving the parenchyma often require a broader differential diagnosis. For instance, the classic symmetrical sclerosis of long bones is virtually pathognomonic for Erdheim-Chester disease. Histology shows a vaguely nodular lesion with a mixed inflammatory infiltrate that is often plasma cell rich and includes large pale "ganglioid" histiocytic cells with emperipolesis (CE, H & E). The presence of occasional hyperplastic meningothelial nests (C, upper left) may promote a misdiagnosis of "lymphoplasmacyte-rich meningioma. The inflammatory infiltrate is polyclonal and represents a reactive process rather than a true neoplasm. Sparse lymphoplasmacytic infiltrates, eosinophils, and surrounding fibrosis are also common. Neurologic involvement is present in 30% of cases and is virtually always associated with nonneurologic symptoms, most commonly bone pain. The diagnosis is typically made based on associated classical clinical and radiographic patterns of systemic involvement. Erdheim-Chester disease is typically progressive, and the prognosis is poor-most patients succumb to their disease within a few years of initial presentation. Histiocytic sarcomas are characterized by cytologic atypia, necrosis, and high proliferative activity. The clinical course for the few reported cases to date has been aggressive and typically fatal. Primary central nervous system lymphomas and related diseases: pathological characteristics and discussion of the differential diagnosis. Marginal zone dural lymphoma: the Memorial Sloan Kettering Cancer Center and University of Miami experiences. Primary central nervous system lymphoma can be histologically diagnosed after previous corticosteroid use: a pilot study to determine whether corticosteroids prevent the diagnosis of primary central nervous system lymphoma. The Influence of Corticosteroids on Diagnostic Accuracy of Biopsy for Primary Central Nervous System Lymphoma. Demyelination as a harbinger of lymphoma: a case report and review of primary central nervous system lymphoma preceded by multifocal sentinel demyelination. Clinical and radiographic spectrum of pathologically confirmed tumefactive multiple sclerosis. The safety of resection for primary central nervous system lymphoma: a single institution retrospective analysis. Rosai-Dorfman disease involving the central nervous system: seven cases from one institute. Disseminated intracranial xanthoma disseminatum: a rare case report and review of literature. Juvenile xanthogranulomas of the nervous system: a report of two cases and review of the literature. Population-based experience on primary central nervous system lymphoma 2000-2012: the incidence is increasing. Trends in primary central nervous system lymphoma incidence and survival in the U. Primary central nervous system lymphoma: the Memorial Sloan-Kettering cancer center prognostic model. Intraoperative neurocytology of primary central nervous system neoplasia: a simplified and practical diagnostic approach. Primary low-grade diffuse small lymphocytic lymphoma of the central nervous system. Primary Burkitt lymphoma of the fourth ventricle mimicking a medulloblastoma in a child. Primary malignant lymphoma of the central nervous system in an immunocompetent child: a case report. Primary T cell central nervous system lymphoblastic lymphoma in a child: case report and literature review. That, and the notion that the germ cell theory employs parthenogenesis in humans, and the lack of a plausible explanation of the mechanism through which primordial germ cells mismigrate to the cranial cavity, led to its challenge by Sano and colleagues who proposed the alternative "embryonic cell theory. It additionally provides a thorough review of a wide range of helpful immunohistochemical markers in the study of this complex group of tumors. The most common differential diagnostic considerations and how to resolve them are discussed, and this is supplemented by a table summarizing the most useful immunohistochemical markers for each subtype. The close resemblance of the methylation pattern of pure germinomas to that of primordial germ cells suggests a possible pathogenetic association. Male predominance is maintained throughout all histologic subtypes, being most pronounced in teratomas and least recorded in germinomas. They are most common in Far East Asia and Japan where they represent up to 15% of all pediatric brain tumors, but are relatively infrequent in the Western Hemisphere where they account for only 0. Massive intracranial or so-called holocranial variants, usually in the form of congenital teratomas, are rarely encountered. Pineal region tumors produce symptoms stemming from either aqueductal compression (increased intracranial pressure) or distortion of the quadrigeminal plate (mental status changes, upward gaze palsies and convergence-Parinaud syndrome). The triad of diabetes insipidus, loss of visual acuity, and hypopituitarism is characteristic of suprasellar tumors. Heterogeneous contrast enhancement is noted on a postcontrast sagittal sequence (C). Calcification is frequently observed in pineal tumors, but hemorrhage is exceptional and suggests the diagnosis of choriocarcinoma.
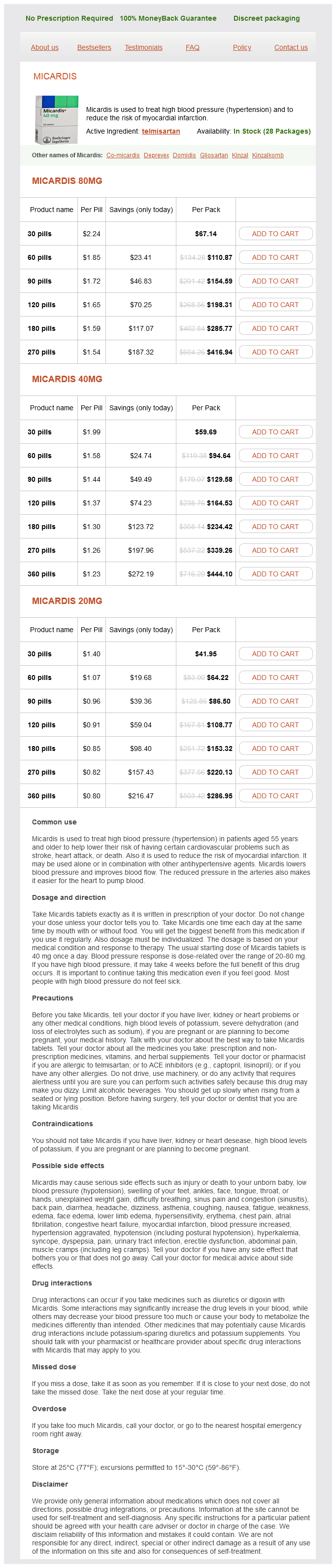
Telmisartan Dosage and Price
Micardis 80mg
- 30 pills - $67.14
- 60 pills - $110.87
- 90 pills - $154.59
- 120 pills - $198.31
- 180 pills - $285.77
- 270 pills - $416.94
Micardis 40mg
- 30 pills - $59.69
- 60 pills - $94.64
- 90 pills - $129.58
- 120 pills - $164.53
- 180 pills - $234.42
- 270 pills - $339.26
- 360 pills - $444.10
Micardis 20mg
- 30 pills - $41.95
- 60 pills - $64.22
- 90 pills - $86.50
- 120 pills - $108.77
- 180 pills - $153.32
- 270 pills - $220.13
- 360 pills - $286.95
Atypical pituitary adenomas: incidence blood pressure solution scam 80 mg telmisartan with amex, clinical characteristics, and implications. Protocol for the examination of specimens from patients with primary pituitary tumors. The complementary role of transcription factors in the accurate diagnosis of clinically nonfunctioning pituitary adenomas. Growth hormone tumor histological subtypes predict response to surgical and medical therapy. Reassessment of the role of radiation therapy in the treatment of endocrine-inactive pituitary macroadenomas. Null cell adenomas of the pituitary gland: an institutional review of their clinical imaging and behavioral characteristics. Clinicopathological features of growth hormone-producing pituitary adenomas: difference among various types defined by cytokeratin distribution pattern including a transitional form. Adenoma granulation pattern correlates with clinical variables and effect of somatostatin analogue treatment in a large series of patients with acromegaly. Silent subtype 3 pituitary adenomas are not always silent and represent poorly differentiated monomorphous plurihormonal Pit-1 lineage adenomas. Suprasellar adrenocorticotropic hormone-secreting ectopic pituitary adenoma: case report and literature Review. Ectopic pituitary adenoma of the clivus presenting with apoplexy: case report and review of the literature. Spectrum of different types of hypophysitis: a clinicopathologic study of hypophysitis in 31 cases. Nuclear beta-catenin accumulation associates with epithelial morphogenesis in craniopharyngiomas. Spindle cell oncocytomas and granular cell tumors of the pituitary are variants of pituicytoma. Intrasellar and suprasellar schwannoma misdiagnosed as pituitary macroadenoma: a case report and review of the literature. Computed tomography and magnetic resonance imaging findings of intrasellar schwannoma: a case report and literature review. Schwannoma in sellar region mimics invasive pituitary macroadenoma; literature review with one case report. Atypical teratoid/rhabdoid tumor in the sella turcica of an elderly female with a distinct vascular pattern and genetic alterations. Sella turcica atypical teratoid/rhabdoid tumor complicated with lung metastasis in an adult female. Adult variant of atypical teratoid/rhabdoid tumor: immunohistochemical and ultrastructural confirmation of a rare tumor in the sella tursica. Other factors that alter risk of toxicity include the specific therapeutic modality and dosage, single therapy versus combined radiation and chemotherapy, genetic background, and idiosyncratic reactions. Introduction Although pathologists typically focus their attention nearly exclusively on the neuropathologic changes of natural disease, therapy-associated neuropathology is increasingly playing a role, particularly now that posttherapy biopsies have become common. To avoid misdiagnosing a host of primary pathologic changes, such as tumor necrosis, vasculopathies, demyelination, cerebral infarction, inflammatory conditions, vasculitis, and others, it is critical to recognize iatrogenic changes induced by prior surgery, intravascular embolization (see Chapter 13), electrode placement (see Chapter 25), chemotherapy, and, especially, radiation therapy. Surgical complications are usually acute and consist mostly of hemorrhage, vascular damage, infarcts, coagulopathies, malignant cerebral edema with herniation, and postoperative infection. Similarly, preoperative tumor embolization has acute complications, such as infarct and hemorrhage. In neuropathology, post-embolization specimens are mainly encountered in the setting of large hypervascular meningioma resections, in which intratumoral necrosis and reactive changes are most commonly noted. Similarly, the side effects of therapy on the peripheral nervous system are not covered. The most serious side effects of radiation and chemotherapy, such as radiation necrosis, chemotherapy-associated leukoencephalopathy, and secondary neoplasms, are mostly chronic or remote in nature, often manifesting years after therapy. Some patients suffer to a much greater extent than others from therapy-induced neurotoxicity, although individual risks are difficult to predict. Nonetheless, the actively developing central nervous system appears to be particularly vulnerable, especially to radiation. A range of milder and sometimes reversible forms of damage are often managed by oncologists. A variety of vascular changes due to radiation are lumped together under the heading of radiation vasculopathy, whereas a more diffuse form of white matter damage known as radiation leukoencephalopathy is usually encountered in the setting of large volume or whole brain therapy, although postradiosurgery examples have also been reported. Brief Historical Overview Injury to the nervous system is a common complication of radiation therapy, which was classically divided into acute, early delayed, and late delayed forms by Dr. In contrast, late delayed effects typically occur years after 493 Therapy-Associated Neuropathology Abstract Now that post-therapy biopsies have become increasingly common, it is critical to distinguish therapy-induced changes from native pathology, including tumor necrosis, demyelination, cerebral infarction, inflammatory conditions, vasculitis, and others. The very therapies employed to enhance survival and quality of life can also be neurotoxic. Therefore this chapter highlights the diagnostic changes associated with radiation necrosis, non-necrotizing radiation injuries, therapy-induced leukoencephalopathies and vasculopathies, and secondary neoplasms after therapy. Infants and young children are even more vulnerable and generally, the younger the patient, the higher the risk of radiation-induced damage. Subcortical U fibers are often spared, although lesions can extend into the adjacent cortex or deep gray matter. Microscopically, small to midsize vessels show the most impressive pathologic changes, providing at least one potential explanation for the subcortical predilection. Radiation necrosis versus tumor recurrence is an extremely common differential diagnosis in post-therapy biopsy specimens (Table 21. Most commonly, there is a mixture of both residual/recurrent tumor and radiation necrosis, and some data suggest that the ratio of the two provides meaningful prognostic information. Also, the post-therapy tumor sometimes appears cytologically inert or "stunned" and it is difficult to know whether these cells are "coming or going"; in other words, it is not clear if tumor cells would have died given additional time or if they were in an early state of recovery.
© 2025 Adrive Pharma, All Rights Reserved..