General Information about Tastylia
Moreover, Tastylia can be identified for its minimal unwanted aspect effects. In most cases, the one facet effect reported is a mild headache, which is usually temporary and may be easily managed with over-the-counter painkillers. This is as a outcome of the treatment is absorbed immediately into the bloodstream, reducing the probabilities of gastrointestinal side effects generally seen with different ED medicines.
If you're one of many tens of millions of males battling erectile dysfunction (ED), you know the way irritating and embarrassing it may be. ED is a common situation that impacts many men, causing difficulties in achieving and sustaining an erection. Fortunately, there are therapies available that can assist males overcome this drawback and regain their confidence in the bedroom. One such resolution is Tastylia – a novel and effective treatment for ED that has been garnering consideration and impressive outcomes.
One of the most important benefits of utilizing Tastylia is its ability to provide longer-lasting results. Many males who've tried this treatment have reported being in a position to obtain and keep an erection for longer intervals of time, giving them and their partners a more satisfying and pleasurable sexual expertise. This is as a end result of Tadalafil stays within the physique for a longer length than other ED drugs, allowing males to be extra spontaneous in their sexual activities.
In conclusion, Tastylia has emerged as a game-changer in the world of ED treatments. Its distinctive oral strips and quicker onset of motion have made it a preferred choice for so much of males battling this condition. With its impressive outcomes and minimal unwanted effects, it has confirmed to be a safe and efficient possibility for enhancing sexual performance. However, as with any treatment, you will want to consult with a healthcare professional earlier than beginning any new therapy.
In addition to its effectiveness in treating ED, Tastylia is also gaining recognition amongst men because of its discreetness. The oral strips are small and discreetly packaged, making it easy to take them on-the-go without anybody figuring out. This offers a more handy and comfortable option for men who may really feel embarrassed about their situation.
The results of Tastylia could be seen inside 15-20 minutes of consumption, a lot faster than conventional ED drugs. This is as a outcome of the treatment is absorbed instantly into the bloodstream via the tissues in the mouth, bypassing the digestive system. This permits for faster onset and longer duration of motion, with Tastylia being effective for up to 36 hours.
Tastylia has been confirmed to be efficient in treating all types of ED, including psychological and bodily causes. It has also been found to be useful for males with diabetes and different medical conditions that may contribute to ED. This makes it a viable option for a wider range of males who might have beforehand been unable to find a suitable therapy for his or her condition.
Tastylia comes within the form of oral strips that dissolve on the tongue. These strips contain a drugs called Tadalafil, which belongs to a class of medicine generally identified as PDE-5 inhibitors. Tadalafil works by growing the blood flow to the penis, which helps in achieving and sustaining an erection. The strips are placed on the tongue and dissolve inside seconds, making it a discreet and handy type of therapy.
Which part of the label you expect to be mostly likely revised with more phase 4 information Where would you find information concerning the safety of this drug in pregnant women Whole blood samples are generally harder to process and assay than serum or plasma samples symptoms 6 days after iui discount 10 mg tastylia amex. Plasma may be considered a liquid tissue compartment in which the drug in the plasma fluid equilibrates with drug in the tissues and cellular components. At what time intervals should plasma drug concentration be taken in order to best predict drug response and side effects The time needed for the drug to reach the site of action, produce a pharmacodynamic effect, and reach equilibrium are deduced from studies on the relationship of the time course for the drug concentration and the pharmacodynamic effect. Often, the drug concentration is sampled during the elimination phase after the drug has been distributed and reached equilibrium. For multiple-dose studies, both the peak and trough drug concentrations are frequently taken. What are the reasons to use a multicompartment model instead of a physiologic model Missing information in the physiologic model will lead to bias or error in the model. Compartment models are more simplistic in that they assume that both arterial and venous drug concentrations are similar. The compartment model accounts for a rapid distribution phase and a slower elimination phase. Physiologic clearance models postulate that arterial blood drug levels are higher than venous blood drug levels. Organ drug clearance is useful in the treatment of cancers and in the diagnosis of certain diseases involving arterial perfusion. The plasma drug leveltime curve describes the pharmacokinetics of the systemically absorbed drug. The purpose of pharmacokinetic models is to relate the time course of the drug in the body to its pharmacodynamic and/or toxic effects. The pharmacokinetic model also provides a basis for drug product design, the design of dosage regimens, and a better understanding of the action of the body on the drug. Several different experimental conditions are needed to prove which of the above hypotheses is the most likely cause for C1 > C2. These experiments may use in vivo or in vitro methods, including intracellular electrodes to measure pH in vivo, protein-binding studies in vitro, and partitioning of drug in chloroform/water in vitro, among others. In the case of protein binding, the total concentration of drug in each compartment may be different (eg, C1 > C2) and, at the same time, the free (nonprotein-bound) drug concentration may be equal in each compartment-assuming that the free or unbound drug is easily diffusible. Similarly, if C1 > C2 is due to differences in pH and the nonionized drug is easily diffusible, then the nonionized drug concentration may be the same in each compartment. The total drug concentrations will be C1 = C2 when there is similar affinity for the drug and similar conditions in each compartment. The total amount of drug, A, in each compartment depends on the volume, V, of the compartment and the concentration, C, of the drug in the compartment. Since the amount of drug (A) = concentration (C) times volume (V), any condition that causes the product, C1V1 C2V2, will result in A1 A2. However, as more information becomes available through postmarketing commitment studies, more information is added to the labeling, including Warnings and Precautions. An excipient such as aspartame in a product is mostly found under the Description section, which describes the drug chemical structure and the ingredients in the drug product. Section 8, Use in Specific Populations, reports information for geriatric, pediatric, renal, and hepatic subjects. Kawai R, Mathew D, Tanaka C, Rowland M: Physiologically based pharmacokinetics of cyclosporine. Integration of Pharmacokinetics, Pharmacodynamics and Toxicokinetics in Rational Drug Development. Sawada Y, Hanano M, Sugiyama Y, Iga T: Prediction of the disposition of nine weakly acidic and six weekly basic drugs in humans from pharmacokinetic parameters in rats. Benowitz N, Forsyth R, Melmon K, Rowland M: Lidocaine disposition kinetics in monkey and man. Chiou W: Quantitation of hepatic and pulmonary first-pass effect and its implications in pharmacokinetic study, I: Pharmacokinetics of chloroform in man. Cowles A, Borgstedt H, Gilles A: Tissue weights and rates of blood flow in man for the prediction of anesthetic uptake and distribution. Gibaldi M: Estimation of the pharmacokinetic parameters of the two-compartment open model from post-infusion plasma concentration data. Lutz R, Dedrick R, Straw J, et al: the kinetics of methotrexate distribution in spontaneous canine lymphosarcoma. Montandon B, Roberts R, Fischer L: Computer simulation of sulfobromophthalein kinetics in the rat using flow-limited models with extrapolation to man. Rowland M, Thomson P, Guichard A, Melmon K: Disposition kinetics of lidocaine in normal subjects. Calculus is an important mathematic tool for analyzing drug movement quantitatively. Differential equations are used to relate the concentrations of drugs in various body organs over time. Integrated equations are frequently used to model the cumulative therapeutic or toxic responses of drugs in the body. Represent pharmacokinetic data graphically using Cartesian coordinates (rectangular coordinate system) and semilogarithmic graphs.
Treatment to elevate the platelet count may become necessary if the level drops to < 50 Â 109/L treatment keratosis pilaris purchase tastylia now. The decision to induce labour or to perform a caesarean section is usually made for obstetric reasons alone. A platelet count should be checked 6 weeks postpartum to ensure that it has returned to normal. If this does not occur, the general practitioner should refer the patient to a haematologist for further assessment. At delivery, an umbilical cord blood sample should be taken to obtain a platelet count, which should also be monitored 25 days after delivery, as this is when a nadir is often seen. The purpose of including this condition is that it is an important diagnosis to make because the untreated mortality is 90% half of which occurs within 24 hours of presentation. Maternal antibodies to the fetal antigens cross the placenta and bind to fetal platelets, causing fetal thrombocytopenia. With each successive pregnancy, thrombocytopenia occurs at earlier gestation and tends to be more severe. The diagnosis is confirmed after maternal and paternal platelet typing reveals that the father has a platelet antigen that the mother lacks and the mother has detectable antibodies to this antigen. More recently the invasive option of serial intravascular fetal platelet transfusions is being superseded by conservative therapy employing maternal intravenous immunoglobin infusions, alone or in combination with oral prednisolone therapy. Pregnancy itself is a thrombophilic state due to an increase in clotting factors and decrease in naturally occurring anticoagulants. It does not deal with the diagnosis and treatment of venous thromboembolism in pregnancy but gives a framework for managing women who have been diagnosed with a thrombophilia. The predisposition to thrombosis is not unique to laboratory-reported thrombophilia. Many other predispositions to thrombosis exist, and these are outlined in Table 7. Caesarean section is a risk, but women who deliver vaginally may also be at risk and this must not be overlooked. Patients may have a diagnosis of an acquired or inherited thrombophilia made following investigations for adverse pregnancy outcome, criteria for which are detailed in Table 7. It is prudent to obtain a thrombosis history to be able to decide on whether thromboprophylaxis is indicated and the length of thromboprophylaxis. One or more unexplained deaths of a morphologically normal fetus at or beyond the 10th week of gestation. One or more preterm births of a morphologically normal neonate before the 34th week of gestation because of (i) eclampsia or severe pre-eclampsia or (ii) recognized features of placental insufficiency. Three or more unexplained consecutive spontaneous miscarriages before the 10th week of gestation, with maternal anatomic or hormonal abnormalities and paternal and maternal chromosomal cause excluded. The primary antiphospholipid syndrome is diagnosed when at least one clinical criterion and laboratory criteria are met. Women with three or more risk factors should be considered for thromboprophylaxis antenatally. Women with two or more persisting risk factors should be considered for thromboprophylaxis for at least 7 days postpartum. Key summary points · · · · · An acute sickle cell painful episode should be treated as a medical emergency with the aim of achieving effective pain control both promptly and safely. Positive screening and carrier results for the England-wide universal newborn sickle cell screening programme by ethnicity and area for 200507. Clinical outcomes in children with sickle cell disease living in England: a neonatal cohort in East London. Sickle Cell Acute Painful Episode: Management of an Acute Painful Sickle Cell Episode in Hospital. Idiopathic thrombocytopenic purpura: a practice guideline developed by explicit methods for the American Society of Hematology. Guidelines on the diagnosis and management of thrombotic thrombocytopenic purpura and other thrombotic microangiopathies. A screening and intervention program aimed to reduce mortality and serious morbidity associated with severe neonatal alloimmune thrombocytopenia. The commonest malignancies encountered in pregnancy are cervical, breast, melanoma, ovarian and acute leukaemia. Diagnosis of a malignancy may occur later than in the non-pregnant woman, resulting in more advanced stage of disease at diagnosis, although in general the course of the malignancy does not appear to be affected by pregnancy. The presence of cancer in itself does not affect fetal wellbeing, although the fetus may need to be delivered prematurely to facilitate commencement of maternal treatment, and the long-term health and wellbeing of the mother should be prioritized over that of the fetus. Following a cervical smear test, a woman who meets the criteria for colposcopy still needs colposcopy if she is pregnant. The primary aim is to exclude invasive disease and to defer biopsy/ treatment of pre-invasive disease until the woman has delivered. If invasive disease is suspected clinically or colposcopically, a biopsy adequate to make the diagnosis is essential. Cone, wedge and diathermy loop biopsies in pregnancy are all associated with a risk of haemorrhage of approximately 25%. Treatment of cervical cancer will depend on the staging at diagnosis and the gestation of the pregnancy. Specialist advice and intensive discussions with the woman are needed to determine the appropriate balance between early treatment and a successful pregnancy outcome.
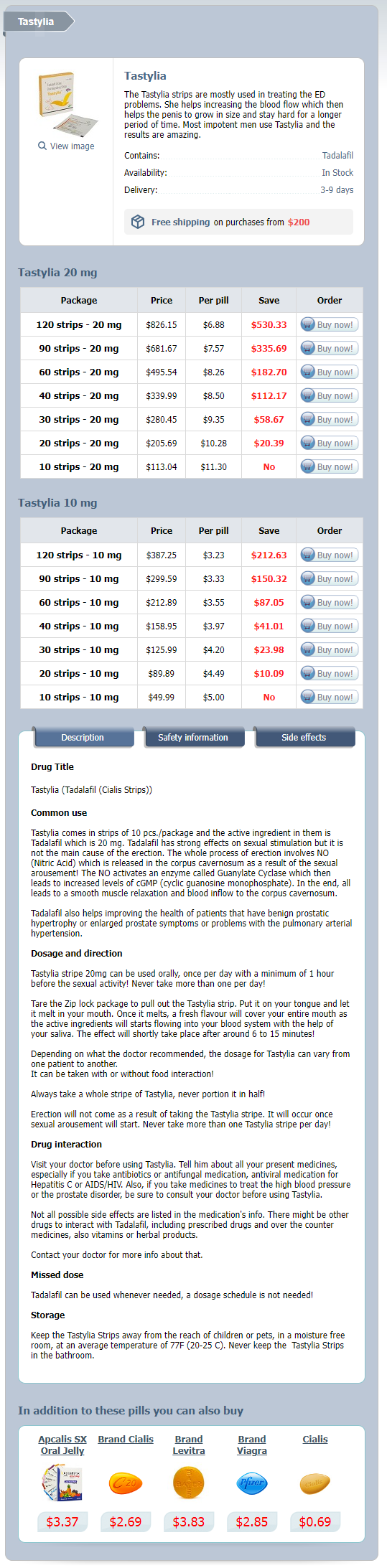
Tastylia Dosage and Price
Tastylia 20 mg
- 120 strips - $826.15
- 90 strips - $681.67
- 60 strips - $495.54
- 40 strips - $339.99
- 30 strips - $280.45
- 20 strips - $205.69
- 10 strips - $113.04
Tastylia 10 mg
- 120 strips - $387.25
- 90 strips - $299.59
- 60 strips - $212.89
- 40 strips - $158.95
- 30 strips - $125.99
- 20 strips - $89.89
- 10 strips - $49.99
The cost of a second oligonucleotide drug treatment 2nd 3rd degree burns tastylia 10mg purchase on line, Macugen, has made the treatment prohibitive given the availability of cheaper, equally effective drugs. Both drugs act locally (in the eye) but several other antisense drugs administered intravenously have also been approved such as Alicaforsen and Mipomirsen. For this approach to be useful, the etiology and genetics of the disease must be known. For example, in the case of viral infection, known sequences belonging to vital genes can be targeted and inhibited by antisense drugs. Many antisense sequences are usually tested to find the best candidate, since intra- and intermolecular interactions can affect oligonucleotide activity and delivery. Antisense and gene therapy approaches have also been combined using viral vectors to deliver an antisense sequence. Frequently Asked Questions »» What is the most frequent route of administration of biologic compounds These substances hold great potential for more specific drug action with fewer side effects. However, many naturally produced substances are complex molecules, such as large-molecular-weight proteins and peptides. Conventional delivery of protein and peptide drugs is generally limited to injectables and implantable dosage forms. Insulin pumps for implantation have been developed for precise control of sugar levels for diabetes, as well as other novel delivery methods such as inhalers such as Afrezza, which delivers rapid acting insulin to the lung. Formulating protein drugs for systemic use by oral, or even any extravascular, route of administration is extremely difficult due to drug degradation and absorption from the site of administration. Designing, evaluating, and improving protein and peptide drug stability is considerably more complex than for small conventional drug molecules. A change in quaternary structure, such as aggregation or deaggregation of the protein, may result in loss of activity. Changes in primary structure of proteins frequently occur and include deamidation of the amino acid chains, oxidation of chains with sulfhydryl groups, and cleavage by proteolytic enzymes present throughout the body and that may be present due to incomplete purification. Proteins may also have a high allergenic or immunogenic potential, particularly when nonhuman genes or production cells are used. Because of the many stability and delivery problems associated with protein and nucleic acid drugs, new delivery systems are being tested to improve their in vivo properties. Carriers can be used to protect the drug from degradation, improve transport or delivery to cells, decrease clearance, or a combination of the above. In this chapter, carriers used for both small traditional drug and biopharmaceutical drug delivery are reviewed. Carriers may be covalently bound to the drug, where drug release is usually required for pharmacologic activity. Polymeric Delivery Systems Polymers can be designed to include a wide range of physical and chemical properties and are popularly used in drug formulations because of their versatility. Polymers initially were used to prolong drug release in controlled-release dosage forms. The development of site-specific polymer or macromolecular carrier systems is a more recent extension of earlier research. In the case of polymeric prodrugs, a spacer group may be present, bridging the drug and the carrier. The spacer chain may influence the rate at which the drug will hydrolyze from the prodrug system. At present, most site-specific polymeric drug carriers are limited to parenteral administration and primarily utilize soluble polymers. An added advantage of complexed cationic polymers is that targeting agents such as receptor ligands can be covalently attached to the polymer rather than the drug to provide cell-specific targeting. Cationic polymer use in vivo is limited because of polymer toxicity, stability, efficacy, and dissociation of the complex. Polymers may also be covalently conjugated to drugs to improve their solubility or pharmacokinetic properties. Polymers with molecular weights greater than 3050 kDa bypass glomerular filtration, thereby extending the duration of drug circulation in the body. Drugs with a free amino or hydroxyl group may be linked chemically to hydroxyl groups in dextrans by activation of the dextran with periodate, azide, or other agents. The molecular weight of the polymer carrier is an important consideration in designing these dosage forms. Generally, large-molecular-weight polymers have longer residence time and diffuse more slowly. However, large polymers are also more prone to capture by the reticuloendothelial system. For example, exposed galactose residues are recognized by hepatocytes, whereas mannose or l-fructose is recognized by surface receptors in macrophages. In addition to use as regular carriers, polymers may also be formulated into microparticles and nanoparticles. In such delivery systems, the therapeutic agent is encapsulated within a biodegradable polymeric and/or lipid colloidal particle that is in the micrometer or nanometer size range, respectively. Micro- and nanosphere formulations are useful for solubilizing poorly soluble drugs, improving oral bioavailability, protecting against degradation, or providing sustained drug delivery.
© 2025 Adrive Pharma, All Rights Reserved..