General Information about Speman
In conclusion, Speman is an all-natural herbal supplement with quite a few benefits for male reproductive well being. It helps enhance sperm depend, motility, and high quality, and can even enhance libido and sexual efficiency. Additionally, it's protected and freed from side effects, making it a preferred selection for men battling fertility issues. However, it's essential to seek the advice of a healthcare professional before beginning any new complement to make sure it's suitable for you.
The herbal ingredients in Speman have aphrodisiac properties that assist enhance libido, sexual health, and fertility. The supplement additionally has anti-inflammatory and antioxidant properties, which can protect sperm from injury caused by free radicals. It also nourishes the reproductive organs, making them more healthy and extra efficient in producing and storing sperm.
Enhances antioxidant protection: Free radicals can harm sperm and affect their quality and motility. The antioxidant properties of Speman may help shield sperm from oxidative stress, enhancing their chances of fertilization.
It is essential to consult a physician before taking Speman, especially in case you are on any treatment or have a pre-existing medical condition. The complement just isn't appropriate for pregnant or lactating ladies and should be prevented by children.
Reduces irritation: The anti-inflammatory properties of Speman might help cut back inflammation within the reproductive organs, which can improve the overall well being of the male reproductive system.
Speman primarily works by stimulating the testes to supply healthy and viable sperm. It also enhances the functions of the seminal vesicles and epididymis, which are answerable for storing and transporting sperm.
Improves sperm rely and high quality: The natural elements in Speman have been recognized to boost sperm rely, motility, and morphology. Studies have shown that men who took Speman for six months skilled a big enhance in sperm depend and a better quality of sperm.
Safe and pure: One of the significant advantages of Speman is that it's made from pure herbs and minerals, making it secure for consumption and freed from side effects.
Speman could be taken as a pill, capsule, or syrup, relying on personal choice. The recommended dosage is one pill or capsule twice every day, or as directed by a healthcare skilled. The syrup may be taken in a dose of 5ml twice day by day.
Speman is an ayurvedic natural complement that is primarily used to deal with male infertility. It accommodates a mix of potent herbs and minerals that work together to enhance the quality and amount of sperm in males. The supplement is produced by the famend Himalaya Drug Company, which is well known for its natural and safe merchandise.
Speman is an herbal complement that has gained reputation for its potential to promote spermatogenesis – the process of sperm manufacturing. It is a novel blend of pure herbs and minerals which have been used in Ayurvedic drugs for centuries to enhance male reproductive health. This article will delve into the benefits of Speman and how it works to spice up sperm manufacturing.
Speman is formulated utilizing 44 totally different natural components corresponding to Ashwagandha, Kokilaksha, Vanya Kahu, and Gokshura, amongst others. Each ingredient in Speman has its distinctive benefits and works synergistically to increase sperm production and motility.
Increases libido and sexual performance: Speman incorporates aphrodisiac properties that can improve sexual want and performance. It helps improve testosterone ranges, which play a crucial role in male sexual health.
Sophisticated consolidation radiotherapy to sites of initial bulky disease has been employed prostate 72 discount speman 60 pills with visa. The investigators predicted that moderate dose escalation would increase tumor control by 10% at 5 years. Maximum tolerated doses were determined in a multicenter pilot study as 190% of the standard dose for cyclophosphamide and 200% for etoposide. Radiotherapy was administered to bulky disease at diagnosis or residual disease after eight cycles of chemotherapy. These results were confirmed and became even more significant in a 10-year update analysis of the trial published in 2009. Such dose-response relationships also were observed independently with nitrogen mustard, procarbazine, and vincristine. Chapter 74 Hodgkin Lymphoma: Clinical Manifestations, Staging, and Therapy 1147 acute and late causes of deaths, was 18. Dosage, dose intensity, and total dose are decisive factors when comparing similar drug regimens. It is difficult to predict the relative efficacy of regimens that use different drugs. As mentioned above, Hasenclever proposed a theoretical framework as a first step to accomplish that task. Different drug doses in a regimen are assumed to be roughly additive in an efficacy scale when appropriately weighted. This total dose must be further corrected for different treatment durations, assuming a typical regrowth kinetic for each lymphoma entity. The resulting quantity, the effective dose, is a reasonable first-order predictor of relative treatment efficacy. Role of Radiotherapy in Advanced-Stage Hodgkin Lymphoma Several reports have indicated that patients treated with chemotherapy alone failed to respond or progressed, primarily in previously involved nodal sites. However, the benefits of consolidating radiotherapy must be balanced with the risk for serious side effects, particularly a second malignancy in the irradiated field. To overcome the insufficient power of randomized studies with too few patients to detect a relevant difference, Loeffler and colleagues performed a metaanalysis of 14 studies involving more than 1700 patients. Two study designs were compared; in the additional design, irradiation was added to the same chemotherapy regimen, and in the parallel design, more cycles of chemotherapy were substituted for irradiation. In the parallel design, there was no significant difference in diseasefree survival. An important issue is determining the added efficacy of radiotherapy as adjuvant treatment to modern anthracycline-containing chemotherapy and the added late toxicity of this combined-modality treatment. This important study recruited patients for more than 10 years and completed the accrual with 739 patients in 2000. The added late toxicity associated with irradiation was not evaluated in this report because of the short observation time of 79 months. Ninety-one percent of patients received eight cycles of therapy; 77% were given within 16 days, and 94% were given within 22 days. Twenty-three percent of patients experienced thrombocytopenia, and 65% had anemia, in a few cases necessitating the use of erythropoietin or blood transfusions. Recommendations and Future Directions in Advanced Hodgkin Lymphoma Advanced Hodgkin lymphoma has become a curable disease for the majority of patients. Ongoing well-designed prospectively randomized studies are currently evaluating these two approaches, and valid results will be available in the near future. Both approaches aim at finding the best balance between toxicity and efficacy for the benefit of each individual patient. Unfortunately, both approaches are not tested against each other within a single randomized trial; therefore the current debate on the standard treatment of advanced-stage Hodgkin lymphoma will very likely continue. Early relapses within 12 months of complete remission (approximately 15% of all cases) 3. Late relapses after complete remission lasting longer than 12 months (approximately 15% of all cases) Prognostic Factors for Patients With Primary Progressive Hodgkin Lymphoma Patients with primary progressive disease, defined as progression during induction treatment or within 90 days after the end of treatment, have a poor prognosis particularly when treated with conventional salvage regimens. In a multivariate analysis, Karnofsky performance score at the time to progression (P <0. The survival of these patients is at least equal compared with patients who initially present with advanced disease and receive chemotherapy. Because more aggressive approaches are associated with increased toxicity, an accurate pretreatment prognostic assessment of patients is required to help select the most appropriate therapeutic regimen. Prognostic Factors for Patients Relapsing After Primary Radiotherapy the relapse rate after primary radiation therapy is 30% to 35%, and most relapses occur within 3 years after completion of radiotherapy, although late relapses after 4 years have been observed in 5% to 7% of patients. This small fraction of late disease recurrence is noteworthy because this is generally a more favorable prognostic group when treated with systemic therapy. Most patients who relapse after radiotherapy are treated with systemic combination chemotherapy, often with the inclusion of involved-field radiotherapy if an affected nodal site was previously nonirradiated. The long-term survival of patients varies significantly according to the pattern of relapse. In some series, mixed-cellularity or lymphocyte-depleted histology were also adverse prognostic factors. Prognostic Factors for Early and Late Relapsed Hodgkin Lymphoma Many prognostic factors have been described for patients relapsing after first-line chemotherapy. These include age, gender, histology, relapse sites, stage at relapse, B symptoms, performance status and extranodal relapse. The 5-year failure-free survival rate was 82% for patients lacking all three parameters and 17% for those with one or more risk factors. Three prognostic subgroups were identified according to the presence of the following parameters at relapse: B symptoms, extranodal disease, and initial remission duration of less than 12 months.
They usually occur in patients with focal epilepsy syndromes and with known epilepsy, but occasionally may be a first presentation: 1 prostate cancer 6 on gleason scale buy cheap speman 60 pills on line. Florid psychotic symptoms follow on from a flurry of severe seizures with a consistent time interval, usually 17 days. The episode is usually selflimiting within a week, but may require antipsychotic treatment during that time. Psychotic symptoms occur during the epileptic activity itself, usually as a manifestation of nonconvulsive status epilepticus, and there is evidence of altered awareness. Patients may be agitated and hit out, but directed aggression is exceptionally rare. In both these situations, the best treatment of psychosis is to prevent seizures with antiepileptic therapy. Occurs more often in those with structural lesions (23%) than in mesial temporal sclerosis (5%) and is occasionally caused by antiepileptic drug therapy. Neurological and psychiatric illness may be related in several ways: Neurological diseases may have psychiatric complications. The treatments for psychiatric illnesses can cause neurological complications and vice versa. Psychiatric factors may be important in triggering physical diseases, especially those to which the individual has a predisposition. Psychiatric complications of neurological disease Psychiatric complications of neurological disease may be reactive a response to the handicap of the disease or a primary manifestation of the disease itself. Neurological diseases presenting with psychiatric manifestations Anxiety Anxiety is a common occurrence in neurology outpatients, found in 2535%. The diagnosis of a primary psychiatric illness requires that the symptoms occur in normal consciousness. The presence of altered consciousness or periods of drowsiness suggest a neurological cause (pp. There may, however, be no obvious clouding of consciousness in the early stages and other factors may be helpful in making the diagnosis (Table 1). Anxiety is seen in metabolic encephalopathies, including hypoxia, thyrotoxicosis, delirium tremens and other druginduced states. The aetiology is usually a tumour, infarction, trauma, hydrocephalus, encephalitis or focal dementia. There may be release of primitive reflexes: pout, grasp and palmarmental reflexes. If the lesion extends more posteriorly, there may be more easily identified focal signs: hemiparesis and non-fluent dysphasia in the dominant hemisphere. Disinhibition, with insomnia, hypomanic features and Euphoria, much vaunted, occurs in only 3% of patients with sometimes hypersexuality, is seen in orbitofrontal multiple sclerosis. Visual hallucinations Tactile hallucinations Focal neurological signs Disturbed sleep Paranoia Feelings of control Headache Commonly without auditory hallucinations Commonly without auditory hallucinations Sometimes Reversal of sleep cycle Common Rare Sometimes Rare without auditory hallucinations Rare without auditory hallucinations Rare Insomnia Common Sometimes Sometimes Neurology and psychiatry 2. Apathy, with paucity of speech and motor activity, is seen in mesial frontal lesions, especially bilateral infarction of the anterior cerebral artery. These patients find it difficult to maintain attention or to transfer attention from one task to the next. Auditory hallucinations are common in psychiatric disease and may be accompanied by hallucinations in other modalities, but in organic disease these commonly occur without auditory hallucinations. Visual hallucinations most commonly occur in acute confusional states, where they are often complex (pink elephants in delirium tremens). They may also occur with lesions at any level of the visual system from the eyes to the association cortex, when they may be flashes of light or complex images and may be restricted to an abnormal visual field. Brief, stereotyped images may represent partial seizures but are also seen by normal individuals when falling off to sleep (hypnagogic hallucinations) and, rarely, in brain stem lesions (peduncular hallucinosis). Olfactory, gustatory and somatosensory (crawling ants on the skin) hallucinations also occur in acute organic brain syndromes and in epilepsy (p. While there are several different types of dopamine receptors, allowing some selectivity of action, major side effects of neuroleptic drugs are movement disorders, which may be acute (oculogyric crisis, neuroleptic malignant syndrome) or chronic (tardive movement disorders), whereas the antiparkinsonian drugs cause confusions, hallucinations and psychosis. The characteristic features are muscle rigidity of an extrapyramidal type, altered consciousness and autonomic disturbance, especially hyperpyrexia, which usually develop acutely. It occurs in up to 1% of individuals receiving neuroleptic medication and may occur at any stage during treatment. The diagnosis is made by exclusion of other causes in the appropriate context of neuroleptic therapy. Major complications are renal failure secondary to dehydration, and myoglobinaemia and secondary infection. If the patient can be supported satisfactorily for 1014 days, there are usually no sequelae and neuroleptics have been restarted in some individuals without recurrence. Neurological and psychotropic medication Drugs used in the treatment of psychiatric illness often have neurological side effects and vice versa. Withdrawal of the culprit may not be possible; Table 2 lists some alternative strategies. Most drugs are associated with both neurological and psychiatric complications (Table 3). Neurological causes of acute psychiatric symptoms are similar to those for confusion.
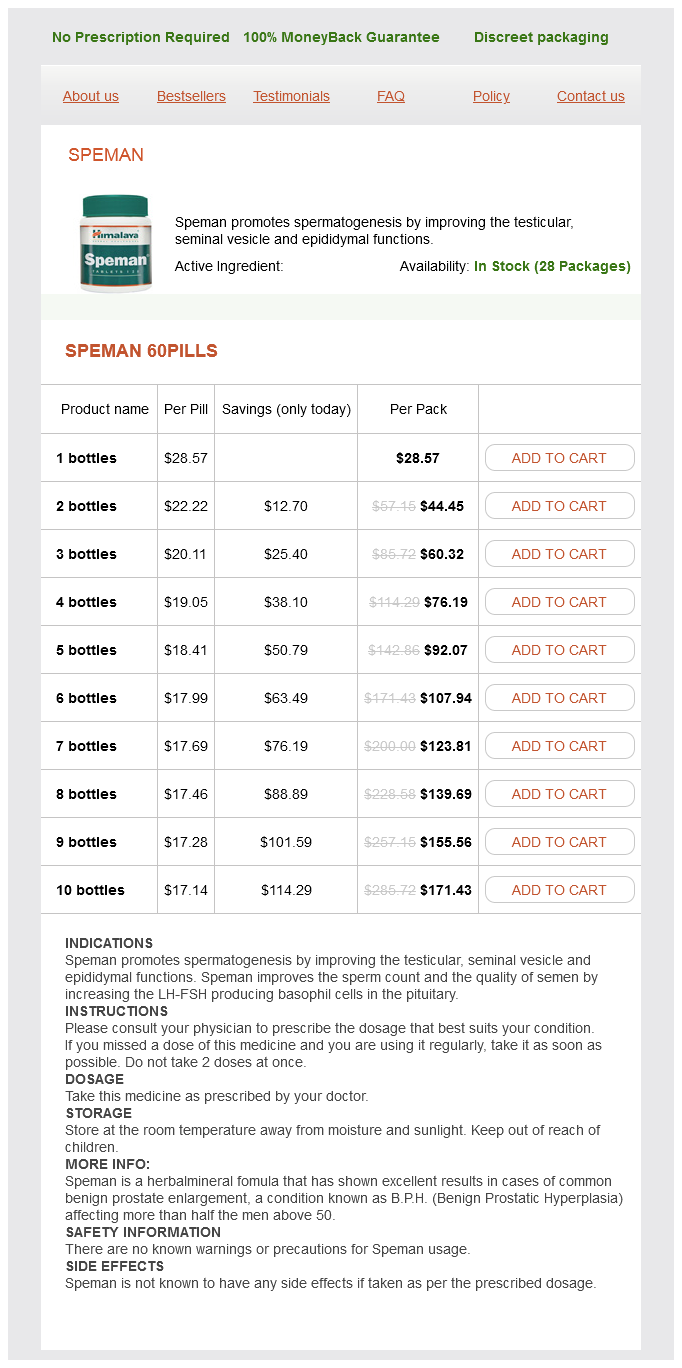
Speman Dosage and Price
Speman 60pills
- 1 bottles - $28.57
- 2 bottles - $44.45
- 3 bottles - $60.32
- 4 bottles - $76.19
- 5 bottles - $92.07
- 6 bottles - $107.94
- 7 bottles - $123.81
- 8 bottles - $139.69
- 9 bottles - $155.56
- 10 bottles - $171.43
The treating physician determines management according to clinical judgment with no prescribed treatment regimen; data are then recorded regarding histology, stage, therapy, response, relapse, and death man health georgia erectile dysfunction gallery 60 pills speman buy mastercard. Thus considerable consultation time is required to review available treatment approaches. The more commonly used regimens in indolent lymphoma cases are shown in Table 79-10. In the absence of a clear standard of care with curative potential, optimal first-line treatment remains enrollment in randomized clinical trials wherever possible. In the National LymphoCare Study,30 academic sites are more likely than community sites to treat patients in clinical trials (12% versus 4% of patients), but it is lamentable that only 6% of patients were enrolled in clinical trials. For patients who are not eligible for clinical trials or who refuse entry, data demonstrate higher response rates, longer duration of responses, and perhaps, improved survival with chemoimmunotherapy. Single-agent monoclonal antibody therapy is appropriate for patients who choose to avoid chemotherapy; this is a reasonable treatment choice based on the results of clinical trials of prolonged or maintenance therapy with rituximab. Optimal results are seen when radioimmunoconjugates are used earlier in the disease course. Data from the National LymphoCare Study29 demonstrate that chemoimmunotherapy is now the treatment of choice of physicians in the United States (see Table 79-9). Significant regional and center differences were observed, strongly suggesting that physician preference is the predominant factor that drives initial therapy. For example, initial "watch and wait" was used in 31% of cases in the Northeast but only in 13% in the Southeast; fludarabine-based chemoimmunotherapy was used in 18% of patients in Southwest but only in 3% in the Northeast. The use of fludarabine in combination with cyclophosphamide is associated with a higher response rate and longer duration of response compared with fludarabine alone in randomized trials. Responding patients were randomized to receive no further therapy or to receive 12 doses (every 8 weeks) for 2 years. Monoclonal Antibody Therapy Monoclonal antibodies are the most exciting agents to emerge in the treatment of indolent lymphomas. Factors associated with lower response rates include chemoresistant disease,55 bulky disease,56 and treatment late in the disease course. Time to next treatment was also longer in the maintenance group than in the observation group. Increased toxicities were seen in the maintenance group, most being infections, but these were largely self-limiting. Conjugated Radiolabeled Monoclonal Antibody Therapy Complexing a radioisotope to a monoclonal antibody (radioimmunoconjugate) might be expected to improve efficacy over antibody therapy alone. Tositumomab complexes 131I (radioactive iodine) to the anti-B1 antibody and has been studied extensively in the treatment of heavily pretreated patients78 and untreated patients,79 as well as for retreatment of indolent lymphomas. The risk for hematologic toxicity increased with dose delivered and with degree of baseline bone marrow lymphoma involvement. Relapsed asymptomatic disease is not necessarily an indication for treatment, and patients can again be managed expectantly. A number of factors must be taken into account in planning therapy; it is not possible to define treatment at relapse without considering the goal of therapy (palliative versus potentially curative), performance status, previous therapy, response, and duration of response. Single-agent rituximab is approved for relapsed lymphoma and is widely used in this setting. The study was closed early because of slow accrual with 140 of the planned 250 patients accrued and only 89 randomized. These include monoclonal antibodies, idiotype vaccines, immunomodulatory agents, and novel kinase inhibitors. These include several humanized antibodies designed to have less infusion toxicity and improved effector function. These agents are now being examined in combination with monoclonal antibodies and chemotherapy. Clinical responses have been observed in a phase I study examining the efficacy of navitoclax in lymphoid malignancies,106 and this agent and similar compounds are currently also being evaluated in ongoing clinical trials alone and in combinations. Federico M, Bellei M, Marcheselli L, et al: Follicular lymphoma international prognostic index 2: A new prognostic index for follicular lymphoma developed by the international follicular lymphoma prognostic factor project. Chapter 79 Clinical Manifestations, Staging, and Treatment of Follicular Lymphoma 1225. Leich E, Salaverria I, Bea S, et al: Follicular lymphomas with and without translocation t(14;18) differ in gene expression profiles and genetic alterations. Karam M, Novak L, Cyriac J, et al: Role of fluorine-18 fluorodeoxyglucose positron emission tomography scan in the evaluation and follow-up of patients with low-grade lymphomas. Solal-Celigny P, Roy P, Colombat P, et al: Follicular lymphoma international prognostic index. Federico M, Bellei M, Marcheselli L, et al: Follicular lymphoma international prognostic index 2: A new prognostic index for follicular 23. Ketterer N, Salles G, Moullet I, et al: Factors associated with successful mobilization of peripheral blood progenitor cells in 200 patients with lymphoid malignancies. Schulz H, Bohlius J, Skoetz N, et al: Combined immunochemotherapy with rituximab improves overall survival in patients with follicular and mantle cell lymphoma: Updated meta-analysis results. Lenz G, Dreyling M, Schiegnitz E, et al: Myeloablative radiochemotherapy followed by autologous stem cell transplantation in first remission prolongs progression-free survival in follicular lymphoma: Results of a prospective, randomized trial of the German Low-Grade Lymphoma Study Group. It is incurable using current approaches and has a poor prognosis after conventional chemotherapy when compared with other types of B-cell lymphomas.
© 2025 Adrive Pharma, All Rights Reserved..