General Information about Rizatriptan
Before using Rizatriptan, it's important to consult a doctor, especially for these with current health circumstances corresponding to coronary heart illness, high blood pressure, or liver problems. Additionally, it is not beneficial for pregnant or breastfeeding women. Like any medicine, there's a danger of experiencing unwanted effects, such as dizziness, dry mouth, flushing, or chest tightness. If any of those side effects persist or worsen, it's critical to hunt medical consideration instantly.
Another benefit of Rizatriptan is its convenience. It is out there in varied types, including tablets, orally disintegrating tablets, and an oral answer, making it simple for patients to take, particularly when experiencing extreme nausea. The orally disintegrating tablets are notably helpful for people who have issue swallowing drugs. Furthermore, Maxalt can be taken with or with out food, making it a flexible possibility for those with busy schedules.
Migraine headaches are a debilitating situation that affects tens of millions of individuals worldwide. They are characterized by severe throbbing pain on one facet of the top, along with different signs such as nausea, sensitivity to mild and sound, and visual disturbances. While there are various medicines available for the remedy of migraines, one drug that has gained important reputation in latest years is Rizatriptan, extra generally generally known as Maxalt.
One of the first advantages of Rizatriptan is its capacity to provide reduction from the ache and symptoms of migraines inside a short period. It has been discovered to be more practical than traditional over-the-counter painkillers, making it a well-liked alternative amongst migraine sufferers. Studies have shown that Rizatriptan can present aid from symptoms such as pain, nausea, and sensitivity to light and sound in as little as two hours, with some experiencing aid in as little as half-hour.
Rizatriptan is a kind of drugs generally known as a triptan, which works by narrowing blood vessels within the mind and lowering inflammation to alleviate migraine symptoms. It is particularly designed to be taken at the onset of a migraine assault, which makes it a fast-acting and efficient therapy possibility for people suffering from this condition.
In conclusion, Rizatriptan, also known as Maxalt, is an efficient and convenient choice for the remedy of migraines. Its fast-acting nature, minimal unwanted facet effects, and completely different forms make it a preferred selection for many patients. However, as with any medication, it is crucial to seek the assistance of a healthcare professional before use and to concentrate on any potential unwanted effects. With correct use and steering from a health care provider, Rizatriptan can provide much-needed aid for those who endure from the debilitating effects of migraines.
One of probably the most important considerations for individuals who endure from migraines is the incidence of unwanted aspect effects. One frequent side impact of migraine treatment is drowsiness, which poses a problem for these who have to go about their day by day activities. However, Rizatriptan has been discovered to have fewer unwanted side effects in comparability with different triptans, making it a better possibility for people who favor a more tolerable treatment.
This will be followed by information on the cellular oxidant defense pathways and the chemical and biochemical basis for their elicitation pain solutions treatment center reviews order 10 mg rizatriptan with mastercard. The importance of regional inhalation dosimetry in these responses will be highlighted. Finally, based on currently available information on the upper respiratory tract reflex and cellular defense pathways, comparisons of the comparative sensitivity of these reflex and cellular defense pathways to oxidant insult will be provided to highlight generalizable response patterns. Sensory innervation of the nose is via the trigeminal nerve with cell bodies in the trigeminal ganglion. The larynx is richly innervated via the recurrent laryngeal nerves and the superior laryngeal nerves with cell bodies primarily in the nodose ganglion. The sensory nerve innervation of the lower respiratory tract is via the vagus, with the nerve cell bodies being located in either the nodose or jugular ganglia. Sensory nerves can be classified either by their morphology (myelinated, nonmyelinated), axon diameter, conduction velocity; physiological function (mechanosensory vs. These are nonmyelinated small diameter nerves that are thought to be the primary chemosensitive nerves in the respiratory tract. The reader is referred to classic (Alarie, 1973; Barnes, 2001) and more recent reviews (Lee and Yu, 2014; Morris, 2010; Sowerwine et al. Stimulation of airway sensory nerves can elicit both respiratory and cardiac responses (Perez et al. It is convenient to consider the reflex responses based on whether they are mediated centrally via the central nervous system or locally within respiratory tissues via neuropeptide release. It should be appreciated, however, that there exists some overlap between these classifications. The precise response is dependent on whether upper respiratory tract trigeminal nerves or lower respiratory tract vagal nerves are stimulated. For inhaled materials the site of nerve stimulation depends on the regional deposition pattern of the irritant. Water-soluble reactive gases and vapors such as chlorine or formaldehyde deposit with near total efficiency in the upper respiratory tract (Morris, 2012) during nose breathing (at reasonably low concentrations) and stimulate trigeminal nerves. Low-solubility vapors, even if reactive, such as ozone, tend to deposit effectively in the lower respiratory tract (Overton et al. For vapors that deposit in both the upper and lower respiratory tract, the trigeminal responses predominate (Alarie, 1973). Acrolein is an 344 Pulmonary Irritant Responses: Oxidants and Electrophiles example of this type of oxidant/electrophilic gas (Morris, 1996; Morris et al. It is important to recognize that unlike the rodent, humans can respire through their mouths. This results in a dramatic alteration in the regional deposition pattern and can make extrapolation of rodent-derived inhalation toxicity data to the human quite difficult (Morris, 2012; Gloede et al. Centrally mediated reflex responses were perhaps most comprehensively described by Alarie (1973) and more recently described by Bessac and Jordt (2010). Stimulation of nasal trigeminal nerves initiates the "sensory irritant" response as termed by Alarie (1973). This is characterized by the sensation of nasal tickling or pain in humans and initiates avoidance behavior. In rodents this response is characterized by a specific change in breathing pattern that is termed "braking" and is observed as a large reduction or cessation of airflow at the onset of each expiration followed by rapid exhalation. This is due to glottal closure followed by the rapid exhalation when the glottis opens (Vijayaraghavan et al. The magnitude of this response can be measured by simply measuring the reduced breathing frequency or by measuring the duration of the "braking" period at the onset of each expiration (Alarie, 1973; Willis et al. This is a complex motor response that involves the lower respiratory tract and larynx. The sensory irritant response is often quantified on the basis of the reduction in breathing frequency that is caused by these materials. Small reductions in breathing frequency due to induction of braking (flow cessation at the start of each expiration) can be demonstrated at much lower concentrations of acrolein (Morris et al. For example, diacetyl vapor, which imparts a buttery flavor and odor, is also a sensory irritant in the rodent. As described by Alarie (1973) stimulation of vagal nerves results in a sensation of breathlessness and/or dyspnea. The precise changes in breathing pattern are time and dose dependent and can include rapid shallow breathing or outright apnea (Alarie, 1973). Stimulation of vagal nerves, in particular the recurrent laryngeal nerve can result in cough, which like sneeze is a complex motor function involving the muscles of the thorax and lower respiratory tract. Afferent sensory nerve stimulation can also result in the centrally mediated activation of parasympathetic efferents. This can result in multiple effects within the lower airways including bronchoconstriction and mucous hypersecretion (Tai and Baraniuk, 2002). Parasympathic-mediated mucous hypersecretion can also occur in the nose (Shusterman, 2007, 2014). This can occur without generation of an action potential that propagates to the central nervous system and is termed antidromal stimulation. The neuropeptides that are released from the nerve endings include substance P, neurokinin A, and calcitonin gene-related peptide. These biologically active peptides can produce multiple responses which tend to be similar in both the upper and lower respiratory tract.
The risk of recurrence after simple aspiration appears to be similar to that after chest drain insertion pain medication for dogs with hip problems rizatriptan 10 mg purchase visa. Simple aspiration can be repeated once if there is unsatisfactory improvement after the first attempt but, if a repeat attempt is also unsuccessful, then the next procedure should be the insertion of a chest drain. Chemical pleurodesis Chemical pleurodesis with talc or other sclerosing agents such as tetracycline can be employed in patients who are not suitable to undergo surgery, due to their comorbid conditions, or are unwilling to undergo the procedure. Although the risk of recurrence with this technique is reduced, it is still higher than the risk after surgery. If aspiration fails, a chest drain should be inserted before clinical deterioration takes place. Indications for surgical intervention the common indications for surgical intervention include failure of re-expansion of lung 5 days after chest drain insertion; second ipsilateral or first contralateral pneumothorax; spontaneous haemopneumothorax; bilateral spontaneous pneumothoraces; and patients working in professions at risk. If pleurodesis is to be performed, this is usually achieved by mechanical pleural abrasion. Patients with tension pneumothorax require urgent insertion of a large-bore cannula into the appropriate intercostal space and, immediately afterwards, insertion of a chest drain. While traditional practice has been to place the cannula in the second intercostal space in the case of tension pneumothorax, a standard cannula may be of insufficient length to reach the pleural space, due to the thickness of the chest wall in this area. Consequently, if this first approach fails, the cannula or chest drain may be inserted in the safe triangle laterally. In most cases, the initial chest drain should be a small-calibre drain, which is usually as effective as a large-bore chest drain and is more comfortable for the patient. A swinging drain indicates that the drain is in the pleural space, while bubbling indicates an ongoing air leak. If the drain does not swing, it is blocked, clamped, or not in the correct position. A bubbling chest drain should never be clamped, as this can result in tension pneumothorax. When a chest drain produces cessation of air leak and full reexpansion of the lung, it is usually removed after a further 24 hours. If the chest drain insertion fails to improve the pneumothorax, after around 48 hours, then low-pressure, high-volume suction should be considered. European Respiratory Society task force statement: diagnosis and treatment of primary spontaneous pneumothorax. Jones Definition of the disease Cystic fibrosis is the most common lethal autosomal recessive disorder in Caucasians. Chronic progressive pulmonary infection and bronchiectasis are the major causes of morbidity and mortality. The disease affects all ductal systems where the basic defect is manifest, including the pancreas, gastrointestinal tract, sinuses, hepatobiliary system, and male reproductive system, and has significant effects on nutrition and growth. Exocrine pancreatic sufficient patients have an improved nutritional status and prognosis but a high incidence of acute and chronic pancreatitis. Gastrointestinal dysmotility is common and may manifest as gastro-oesophageal reflux disease, delayed gastric emptying, reduced small intestinal transit, and reduced large bowel motility. Meconium ileus in infancy, and distal intestinal obstruction syndrome in older patients, are characteristic of cystic fibrosis presenting as small bowel obstruction secondary to the build-up of abnormally viscid material. The inflammatory process is characterized by infiltration of massive numbers of neutrophils into the airways. These release an arsenal of oxidants and proteases which damage the architecture of the lung and further enhance bacterial adhesion. The main bacterial pathogens in early childhood are Staphylococcus aureus and Haemophilus influenza. Abnormal bile salt composition causes cholelithiasis, which is present in approximately 15% of the adult population. Plugging of intra-hepatic bile ducts, with subsequent cirrhosis, portal hypertension, hypersplenism, and risk of variceal bleeding occurs in 2%5% of patients. Nutrition, growth, and bones the poor nutritional state of many cystic fibrosis patients reflects intestinal malabsorption, the increased energy demands resulting from continual respiratory infection, and other factors such as cystic fibrosis-related diabetes and liver disease. Although growth has historically been poor in cystic fibrosis patients, with modern standards of care there is the expectation for normal growth in the vast majority of cystic fibrosis patients. Typical symptoms of the disease, and less common symptoms Although cystic fibrosis is a multisystem disorder, it is respiratory disease that accounts for the majority of the associated morbidity and mortality. Classically, patients have upper lobe bronchiectasis initially, which later becomes widespread. Typical symptoms are dyspnoea, malaise, chronic cough, haemoptysis, and excess purulent sputum production, although sputum retention may occur. Cystic fibrosis-related diabetes Loss of beta cell mass, due to pancreatic destruction, end-organ insulin resistance and delayed absorption causes postprandial hypoglycaemia, impaired glucose tolerance, and overt diabetes mellitus. Approximately 25% of patients over 10 years have cystic fibrosisrelated diabetes, and the incidence rises with age. Cystic fibrosis cases occur in all races, and cystic fibrosis genes are present worldwide but incidence estimates are not available for most non-Caucasian populations. Sinus disease the sinuses are affected in more than 90% of patients, and nasal polyps and nasal obstruction are extremely common. Medical treatment usually meets with limited success, and surgery is often required.
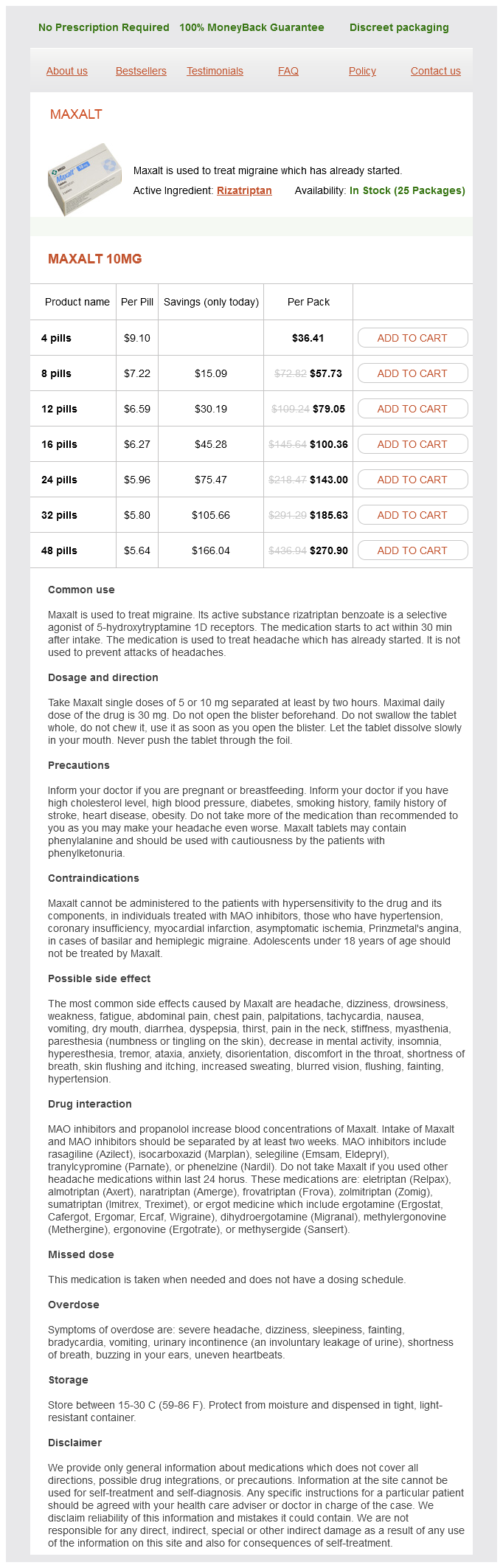
Rizatriptan Dosage and Price
Maxalt 10mg
- 4 pills - $36.41
- 8 pills - $57.73
- 12 pills - $79.05
- 16 pills - $100.36
- 24 pills - $143.00
- 32 pills - $185.63
- 48 pills - $270.90
Renal tract infections or stones should be treated as discussed in Chapters 158 and 166 homeopathic pain treatment for dogs rizatriptan 10 mg buy on line, respectively. In this group, the risk of underlying malignancy is low and the tests are invasive (cystoscopy) and require exposure to ionizing radiation. Prognosis Uncomplicated stones or infections generally have a good prognosis, although patients may suffer from repeated attacks. Renal cell cancers confined to the kidney and completely excised also carry a good prognosis. Microscopic haematuria in association with thin basement membrane disease is a benign condition. However, IgA nephropathy, the major differential diagnosis for thin basement membrane disease, causes progression to end-stage renal disease in up to 40% of patients. How to handle uncertainty in the diagnosis of this symptom the major area of uncertainty is the need for urological investigation in younger patients presenting with microscopic haematuria. Approach to diagnosis the causes of oliguria can be considered anatomically, and divided into prerenal, renal (intrinsic), or post-renal etiologies. Obstructive causes should be excluded early, and the history should focus on symptoms suggesting prostatic disease or bladder or bowel dysfunction. In hospitalized patients, fluid balance, operative notes, and anaesthetic notes should be reviewed, blood pressure recordings checked for episodes of hypotension, and current medications documented. Examination should include an accurate assessment of intravascular fluid balance, focusing on capillary refill, pulse, blood pressure (both supine and standing, if possible), jugular venous pressure, and any evidence of pulmonary oedema. The presence of peripheral oedema does not correlate well with intravascular fluid status. The abdomen should be palpated to exclude an enlarged bladder, and the kidneys balloted. Enlarged kidneys, for example, secondary to hydronephrosis, will sometimes be palpable. If there is a urinary catheter in situ, it should be flushed if there is any concern that it may be blocked. Investigations will be guided by the results of the history and examination, but will usually include a renal tract ultrasound, to exclude significant hydronephrosis or obstruction. For thin individuals, experienced ultrasonographers or radiologists can usually assess renal perfusion and flow characteristics within the renal artery and vein. Differential diagnosis in primary care and secondary care Oliguria can be caused by any factor that affects renal function, or the free passage of urine down the urinary tract. Complete anuria most commonly occurs in men as a consequence of bladder outlet obstruction from an enlarged prostate. It can also arise in patients who have a single functioning kidney which then becomes obstructed or loses its vascular supply. Context Oliguria occurs commonly in hospitalized patients, is usually secondary to impaired renal perfusion, and is often predictable. The elderly and more unwell patients, for example, those in critical care settings, are most at risk. The presence of oliguria tends to reflect the severity of the underlying disease processes. The commonest cause of complete anuria is bladder outflow obstruction from an enlarged prostate. This may be precipitated by prostatitis or constipation in a Specific clues to the diagnosis A palpable bladder or distended bladder on ultrasound suggests an obstructive aetiology. The presence of a rash, neuropathy, or joint involvement, particularly if associated with active urinary sediment. The passage of colacoloured urine (associated with red-cell casts on microscopy), may indicated a rapidly progressive glomerulonephritis. Dipstick evidence of haematuria without the presence of red blood cells on microscopy may represent myoglobinuria; the serum creatinine kinase should be checked. A dipstick urinalysis should always be performed, and the urine should be examined by microscopy and, if appropriate, sent for culture. A renal tract ultrasound will help exclude post-renal causes and can often provide information on renal perfusion. Other diagnostic tests If intrinsic renal disease is suspected, immunological tests should be requested (see Chapter 159) and a renal biopsy may be indicated. Introduction to therapy As the presence of oliguria or anuria is a marker for significant renal disease, initial therapy should be directed at identifying and treating any life threats. Where patients are stable, close observation is indicated, with regular review of fluid balance, urine output, and renal function. Any potentially nephrotoxic medication should be stopped and the doses of other medications adjusted for the degree of renal impairment. The rate of change of renal function with time should be noted, and evidence of ongoing decline or of worsening clinical state should prompt referral to specialist renal services (or intensive care) for consideration of renal replacement therapy if indicated. How to handle uncertainty in the diagnosis of this symptom In many cases, the cause of oliguria is multifactorial. As post-renal causes can usually be readily excluded following examination and an ultrasound if needed, where diagnostic uncertainty persists, management should focus on optimizing renal perfusion and function. This includes avoiding nephrotoxins, preventing obstruction, and supporting renal perfusion, while seeking an underlying cause(s).
© 2025 Adrive Pharma, All Rights Reserved..