General Information about Risperdal
Like any medication, risperidone may trigger unwanted facet effects, similar to drowsiness, dizziness, weight gain, and elevated risk of growing diabetes. It is important to debate any potential unwanted effects with a well being care provider earlier than beginning remedy. Long-term use of this medication may also lead to a serious condition known as tardive dyskinesia (TD), characterized by uncontrollable movements of the face and physique. It is important to often monitor for TD to prevent irreversible injury.
Risperdal is a commonly prescribed medicine for the therapy of schizophrenia, bipolar mania, and irritability associated with autistic dysfunction. Also known by its generic name risperidone, this psychotropic agent has been on the market since 1993 and has been confirmed to successfully manage symptoms related to these circumstances.
The use of risperidone has additionally been controversial, because it has been linked to an elevated danger of strokes and cardiac events, particularly in elderly sufferers with dementia-related psychosis. The U.S. Food and Drug Administration (FDA) has issued a black field warning for these potential risks, and it's crucial to make use of this medicine with warning in this inhabitants.
Risperdal is available in varied varieties, together with tablets, injections, and dissolving tablets, making it a versatile remedy choice for various people' needs. The dosage and size of therapy range and must be determined by a healthcare skilled, bearing in mind an individual's medical history and symptoms' severity.
In conclusion, Risperdal is a well-established medication for the remedy of schizophrenia, bipolar mania, and irritability related to autistic dysfunction. While it could successfully manage signs, it's not a remedy for these conditions. Like any treatment, its use ought to be closely monitored by a healthcare skilled, and any potential unwanted aspect effects or interactions should be discussed overtly. With proper medical care, people can expertise improved quality of life and better administration of their signs with the assistance of risperidone.
Bipolar dysfunction, also known as manic-depressive sickness, is a psychological disorder that causes extreme shifts in moods, vitality and activity ranges. Bipolar mania is the most common type of this dysfunction and is characterised by periods of elevated or irritable moods, increased energy, and impulsive behavior. Risperdal is usually prescribed in conjunction with temper stabilizers to assist manage manic episodes and prevent relapses.
Schizophrenia is a chronic and extreme mental disorder characterized by disordered considering, conduct, and notion of reality. It impacts roughly 1% of the worldwide inhabitants and is often recognized in late adolescence or early adulthood. Individuals with schizophrenia might experience hallucinations, delusions, disorganized considering, and problem with concentration and motivation. Risperdal helps alleviate these symptoms by blocking the activity of dopamine and serotonin, two neurotransmitters concerned in mood regulation and perception.
It is value noting that Risperdal might work together with different medications, together with antibiotics, antidepressants, and antihistamines. It is important to inform a healthcare skilled about any present medicines or supplements earlier than beginning remedy with risperidone.
In recent years, risperidone has additionally gained recognition for its use in treating irritability associated with autistic disorder. Autism spectrum dysfunction (ASD) is a developmental disorder that affects one in 59 youngsters in the United States. Children with ASD usually expertise problem with social interactions, communication, and repetitive behaviors. In some cases, they might also display aggressive and self-injurious behaviors, which may be challenging for folks and caregivers to manage. Risperdal has been proven to minimize back the depth and frequency of these behaviors, improving the general quality of life for these people and their households.
Unopposed estrogen exposure is the underlying cause in the majority of cases of hyperplasia and even most endometrial carcinomas medicine 5 rights generic 2 mg risperdal. This is seen in various clinical situations, including peripheral conversion of androgens to estrogen by adipocytes in obese women or in women who are taking exogenous estrogen without progesterone to help stabilize the endometrium and prevent overgrowth. Vignette 3 Question 4 Answer D: Atypical complex hyperplasia is the most severe form of endometrial hyperplasia. It progresses to carcinoma in approximately answers · 203 the formation of new cysts. Of note, these medications do not treat current cysts, they prevent future cysts by suppressing ovulation. In this clinical setting, expectant management is reasonable but will not help to prevent cyst formation. Surgical removal of the cyst and ovary are much too invasive and are not indicated for a benign functional cyst that is not torsed and is not bleeding. Therefore, most women (75%) using this contraceptive method can still get functional cysts. Women with first-degree relatives (mother or sisters) with endometriosis have a 7% chance of developing the disorder compared to 1% chance in women without a family history. A relationship has also been observed between endometriosis and increased rates of some autoimmune inflammatory disorders such as lupus, asthma, hypothyroidism, chronic fatigue syndrome, fibromyalgia, and allergies. For unclear reasons, endometriosis is identified less often in black and Asian women. Endometrial tissue can be found anywhere in the body, but the most common sites are the ovary and the pelvic peritoneum including the anterior and posterior cul de sacs. Endometriosis in the ovary appears as a cystic collection known as an endometrioma. Other common sites include the most dependent parts of the pelvis such as the posterior uterus and broad ligaments, the uterosacral ligaments, fallopian tubes, colon, and appendix. Although not commonly found, endometriosis has been identified as far away as the breast, lung, and brain. The Halban theory proposes that endometrial tissue is transported via the lymphatic system to various sites in the pelvis, where it grows ectopically. Meyer proposes that multipotential cells in peritoneal tissue undergo metaplastic transformation into functional endometrial tissue. Finally, Sampson suggests that endometrial tissue is transported through the fallopian tubes during retrograde menstruation, resulting in intra-abdominal pelvic implants. A prevailing theory is that women who develop endometriosis may have an altered immune system that is less likely to recognize and attack ectopic endometrial implants. These women may even have an increased concentration of inflammatory cells in the peritoneum that contribute to the growth and stimulation of the endometrial implants. Endometrial implants cause symptoms by disrupting normal tissue, forming adhesions and fibrosis, and causing severe inflammation. Interestingly, the severity of symptoms does not necessarily correlate with the amount of endometriosis. Women with widely disseminated endometriosis or a large endometrioma may experience little pain, whereas women with minimal disease in the cul-de-sac may suffer severe chronic pain. Women with chronic endometriosis and teenagers with endometriosis may not demonstrate this classic pain pattern. Other symptoms associated with endometriosis are dysmenorrhea, dyspareunia, abnormal bleeding, bowel and bladder symptoms, and subfertility. Endometriosis is one of the most common diagnoses in the evaluation of infertile couples. Over 75% of women with symptomatic endometriosis will have pelvic pain and/or dysmenorrhea. Dysmenorrhea usually begins in the third decade, worsens with age, and should raise concern for endometriosis in women who develop dysmenorrhea after years of pain-free cycles. Dyspareunia is usually associated with deep penetration that can aggravate endometrial lesions in the cul-de-sac or on the uterosacral ligaments. Although the exact mechanism is unclear, moderate to severe endometriosis can cause dense adhesions, which can distort the pelvic architecture, interfere with tubal mobility, impair oocyte release, and cause tubal obstruction. Because surgical confirmation is necessary for the diagnosis of endometriosis, the true prevalence of the disease is unknown. It is found almost exclusively in women of reproductive age, and is the single most common reason for hospitalization of women in this age group. Approximately 20% of women with chronic pelvic pain and 30% to 40% of women with infertility have endometriosis. Physical Examination the physical findings associated with early endometriosis may be subtle or nonexistent. To maximize the likelihood of physical findings, the physical examination should be performed during early menses when implants are likely to be largest and most tender. The most common sites (indicated by blue dots) include the ovaries, the anterior and posterior cul de sacs, the uterosacral ligaments, and the posterior uterus and posterior broad ligaments. When the ovary is involved, a tender, fixed adnexal mass may be palpable on bimanual examination or viewed on pelvic ultrasound. Diagnostic Evaluation When the clinical impression and initial evaluation is consistent with endometriosis, empiric medical therapy is often favored over surgical intervention as a safe approach to management.
The ideal correction is based on a line drawn along the first metatarsal that is parallel to the second metatarsal shaft and touches the medial base of the first metatarsal or cuneiform symptoms kidney infection generic risperdal 4 mg buy line. This line crosses the first metatarsal shaft bisector near the ideal location for a corrective osteotomy. The grade of sesamoid subluxation is evaluated to determine whether a lateral capsular release is indicated. Pertinent to the corrective factors of a translational osteotomy is the width of the distal metatarsal. The amount of correction may be limited in a small, narrow, or "hourglass" shaped bone. This additional corrective factor should be addressed during the surgical planning. Correction by lateral translation of the distal metatarsal may be compromised if the cuneiformmetatarsal joint is unstable. The position where this line crosses the first metatarsal bisector helps determine the location and degree of translation needed for the first metatarsal osteotomy. A Freer elevator is helpful to probe and identify the dorsal margin of the subluxed lateral sesamoid. Then incise the capsule longitudinally from the phalanx to well proximal to the lateral sesamoid. The purpose of this longitudinal cut is to allow medialization of the plantar sesamoid complex at the time of capsule repair from the medial side. Mobilize the tissues to expose the capsule from the medial sesamoid inferiorly to the extensor hallucis longus tendon superiorly. The medial plantar digital nerve is also at risk and needs to be protected as the dissection nears the medial sesamoid. Reflect the capsule to expose the medial metatarsal eminence and the joint, but pre- serve it on the dorsal or plantar aspect to minimize risk of vascular insult. Usually the cut is 1 to 2 mm medial to the articular margin or the sagittal groove. If the limbs are too short, there may be instability; if they are too long, there may be difficulty translating or rotating the distal head portion. Next, use a Freer elevator to gently strip the periosteum and soft tissue over the area where the osteotomy is anticipated to cut the dorsal and plantar aspects of the metatarsal. Again, leave the tissues distal to the bone cut in place to minimize vascular compromise. The osteotomy can be affected by saw position with a dorsal, plantar, proximal, or distal angulation. After completing the osteotomy, the distal head fragment should be readily mobilized. Translation is facilitated by applying traction to the toe with one hand and using the other hand to pull with a towel clip on the apex of the proximal metatarsal. If the head fragment is not readily mobilized, the osteotomy needs to be rechecked and cut. Since the osteotomy is usually proximal to the metaphyseal bone, the lateral cortex often appears as a spike. Up to 90% translation is possible and satisfactorily stabilized with Kirschner wires. The osteotomy is translated laterally with traction and thumb pressure on the distal end while counterpressure is applied with a towel clip to the medial spike of the proximal end. The lateral cortex of the proximal metatarsal provides a stable spike to perch the distal head fragment. Pins are typically bent and left out percutaneously but can be cut adjacent to the bone and removed electively. Note contact with the medial and lateral aspect of the proximal metatarsal before entering the distal head fragment. This needs to be contoured in line with the medial metatarsal head to avoid symptoms at this area postoperatively. The amount of tissue removed is judged to allow adequate correction of the hallux valgus. Then perform a "pants-over-vest" closure between the plantar and dorsal capsule to improve sesamoid position. A U-shaped wedge of capsule is removed and sutured to tighten the plantar limb of the capsule and correct the hallux valgus. Suture is placed in a "pants-over-vest" technique to advance the plantar limb of the capsule medial and dorsal. The increased lateral translation of the osteotomy usually decompresses the lateral structures. An aggressive contouring of the proximal portion of the metatarsal is necessary to reduce the risk of a residual bony bump near the osteotomy site. The Kirschner wires need to be placed proximal enough to avoid being cut out during this maneuver. Two Kirschner wires are recommended to reduce the risk of head migration until healing callus has developed. They are allowed to "heel walk" in a postoperative shoe with crutches provided for longer distance or pain management. At 5 weeks the pins are removed and the patient is taught to use a compression wrap and toe spacer. With larger osteotomy translation and correction, radiographic healing can take 3 months or more.
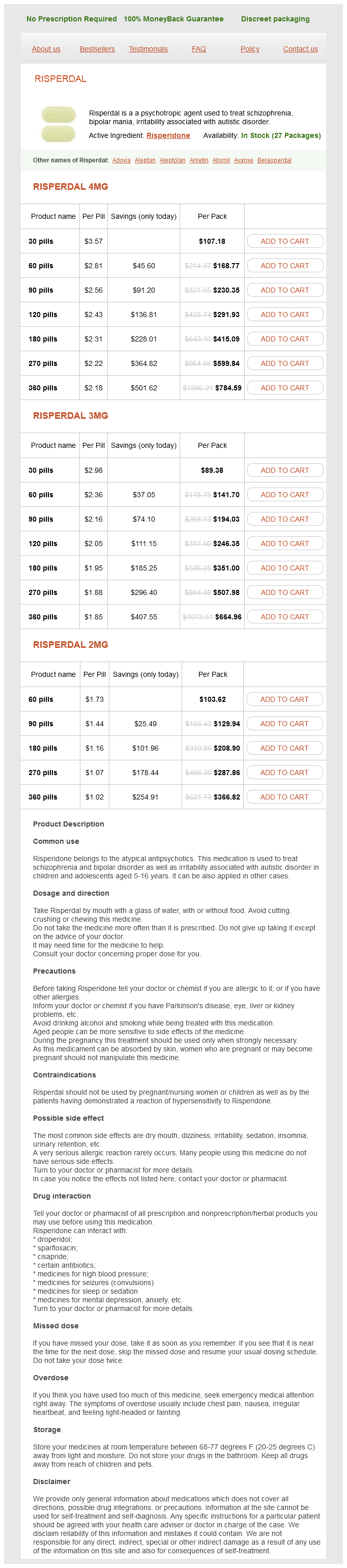
Risperdal Dosage and Price
Risperdal 4mg
- 30 pills - $107.18
- 60 pills - $168.77
- 90 pills - $230.35
- 120 pills - $291.93
- 180 pills - $415.09
- 270 pills - $599.84
- 360 pills - $784.59
Risperdal 3mg
- 30 pills - $89.38
- 60 pills - $141.70
- 90 pills - $194.03
- 120 pills - $246.35
- 180 pills - $351.00
- 270 pills - $507.98
- 360 pills - $664.96
Risperdal 2mg
- 60 pills - $103.62
- 90 pills - $129.94
- 180 pills - $208.90
- 270 pills - $287.86
- 360 pills - $366.82
Factors for choosing the best position include: Gender Occupation Hand dominance Functional requirements Associated joint involvement Unilateral versus bilateral arthrodesis Patient preference One to 3 weeks before surgery medicine of the prophet risperdal 3 mg purchase amex, the elbow to be fused is braced or casted in various angles. Generally acceptable angles include: Male: dominant arm at 90 degrees Females seem to prefer lower angles of 40 to 70 degrees. Bilateral elbow arthrodesis: dominant arm at 110 degrees, nondominant arm at 65 degrees Soft tissue coverage is evaluated. If soft tissue coverage is required, the joint is stabilized with an external fixator. The surgeon should consider bulk graft with demineralized bone matrix and cancellous allograft or autograft. If infection is suspected: Blood work is obtained for complete blood count, sedimentation rate, and C-reactive protein. High-speed burr Power drill Osteotomes Oscillating saw Kirschner wire set Special Instruments Patient Positioning A tourniquet is placed as high on the arm as possible. The patient is placed in the lateral decubitus position with the operative arm resting on a padded arm rest. Identify neurovascular structures in known areas before following structures through areas of heavy scar tissue. Contour the bone so that it can be reduced at the appropriate angle chosen for arthrodesis. It is often necessary to excise the radial head to allow for adequate reduction of the humerus and ulna. The plate is pulled down to the bone and secured with cortical screws before adding locked screws. Check the position and fixation of the construct intraoperatively with fluoroscopy. This is a multiplanar cut and should accommodate for the elbow position in both the coronal and sagittal planes. Intraoperative use of a goniometer to confirm the fusion angle before definitive fixation. Provisional fixation is obtained with Kirschner wires and the fusion position is measured with a goniometer. Keep patients in a cast for at least 4 months, until fusion occurs, depending on radiographs. Intravenous antibiotics are continued for 48 hours or longer, depending on intraoperative cultures. The effect of simulated elbow arthrodesis on the ability to perform activities of daily living. Lateral plantar nerve Plantar Fascia Release in Combination With Proximal and Distal Tarsal Tunnel Release 3911 Chapter 58 Endoscopic Plantar Fasciotomy 3920 Chapter 59 Transection and Burial of Neuromas of the Foot and Ankle 3925 Chapter 60 Barrier Procedures for Adhesive Neuralgia 3933 Chapter 61 Distraction Arthroplasty for Ankle Arthritis 3941 Chapter 62 Supramalleolar Osteotomy With Internal Fixation: Perspective 1 3953 Chapter 63 Supramalleolar Osteotomy With Internal Fixation: Perspective 2 3961 Chapter 64 Supramalleolar Osteotomy With Internal Fixation: Perspective 3 3967 Chapter 65 Supramalleolar Osteotomy With External Fixation: Perspective 1 3976 Chapter 66 k. The chevron osteotomy has become widely accepted for correction of mild and moderate hallux valgus deformities. In the initial reports by Austin and Leventen1 and Miller and Croce,13 no fixation was mentioned. They suggested that the shape of the osteotomy and impaction of the cancellous capital fragment upon the shaft of the first metatarsal provided sufficient stability to forego fixation. To increase the indication for this technically simple osteotomy, internal fixation and a lateral soft tissue release have been added. On the plantar surface of the metatarsal head are two longitudinal cartilage-covered grooves separated by a rounded ridge. The sesamoid bone is contained in each tendon of the flexor hallucis brevis; they are distally attached by the fibrous plantar plate to the base of the proximal phalanx. The head of the first metatarsal is rounded and cartilagecovered and articulates with the smaller concave elliptic base of the proximal phalanx. Fan-shaped ligamentous bands originate from the medial and lateral condyles of the metatarsal head and run to the base of the proximal phalanx and the margins of the sesamoids and the plantar plate. Tendons and muscles that move the great toe are arranged in four groups: Long and short extensor tendons Long and short flexor tendons Abductor hallucis Adductor hallucis Blood supply to the metatarsal head First dorsal metatarsal artery Branches from the first plantar metatarsal artery Hardy and Clapham found in a series of 91 patients a positive family history in 63%. Coughlin2 reported that a bunion was identified in 94% of 31 mothers whose children inherited a hallux valgus deformity. Association of pes planus with the development of a hallux valgus deformity has been controversial. Hohmann was the most definitive that hallux valgus is always combined with pes planus. Coughlin2 and Kilmartin7 noted no incidence of pes planus in the juvenile patient. In this position the foot appears to be less able to withstand the deformity pressures exerted on it by either shoes or weight bearing. The simultaneous occurrence of hallux valgus and metatarsus primus varus has been frequently described. The hallux valgus and intermetatarsal angles and tibial sesamoid position are measured. Spiral dynamics physiotherapy in adolescents Positioning the foot is prepared in the standard manner. The plantar Hohmann retractor protects the plantar artery to the metatarsal head, and the dorsal retractor protects the dorsal intra-articular blood supply originating from the capsule. This is one of the most important principles if a chevron osteotomy is carried out in a moderate to severe deformity. It should be 10 degrees inclined from medial to lateral, and pointing at the head of the fourth metatarsal. In the situation of an elevated position of the first metatarsal, the inclination may be increased. If shortening or lengthening of the first metatarsal is needed, the wire may be aimed to the fifth or third metatarsal head.
© 2025 Adrive Pharma, All Rights Reserved..