General Information about Rabeprazole
In some rare instances, rabeprazole may also trigger more extreme unwanted effects such as allergic reactions, liver damage, and low magnesium ranges. It is necessary to hunt immediate medical consideration should you experience any signs corresponding to difficulty breathing, swelling of the face or throat, yellowing of the pores and skin or eyes, and strange fatigue.
There are some things to bear in mind while taking rabeprazole. It is important to tell your physician in case you have any allergic reactions, medical conditions, or are pregnant or breastfeeding. Rabeprazole could work together with different drugs, so it's essential to tell your physician about any other medications you're taking. It is also beneficial to restrict or avoid alcohol consumption whereas taking rabeprazole, as it can enhance the danger of side effects corresponding to dizziness and drowsiness.
In conclusion, rabeprazole (Aciphex) is an efficient medicine for treating signs of GERD and lowering the amount of acid produced in the abdomen. It is necessary to take the treatment as directed by a physician and to monitor for any potential unwanted effects. By managing and relieving signs of GERD, rabeprazole can enhance an individual's quality of life and forestall potential complications.
GERD is a quite common situation, affecting hundreds of thousands of people worldwide. If left untreated, it may possibly lead to serious issues such as esophageal ulcers, strictures, and even esophageal cancer. The signs of GERD may be quite uncomfortable and can significantly influence a person's day by day life. These signs include heartburn, regurgitation of acid or food, chest ache, difficulty swallowing, and a sour style in the mouth.
Rabeprazole, additionally recognized by its model name Aciphex, is a medicine that is used to reduce the quantity of acid produced in the abdomen. It is usually prescribed for the remedy of gastroesophageal reflux illness (GERD), a condition in which the abdomen acid flows back up into the esophagus, causing harm and discomfort.
Rabeprazole belongs to a category of medicines called proton pump inhibitors (PPIs). PPIs work by blocking the enzyme within the stomach that is answerable for producing acid. By lowering the amount of acid produced within the stomach, rabeprazole helps to alleviate the signs of GERD and permits the esophagus to heal.
Like any medication, rabeprazole could trigger some unwanted effects. These can embody headache, nausea, diarrhea, abdominal ache, and flatulence. However, these side effects are usually mild and will resolve on their own. If they persist or turn into extreme, it's essential to consult with a doctor.
Aciphex is out there in each pill and oral suspension form. It is often taken once a day, with or with out food. The dosage could range relying on the severity of an individual's situation, and it's important to follow the doctor's directions fastidiously. It normally takes a few days of treatment for the medication to begin working, and signs ought to improve inside the first two weeks of beginning the medication. However, it is essential to proceed taking rabeprazole even if signs improve, as stopping the medicine abruptly may cause a rebound impact and make symptoms worse.
By differentiating and treating the shoulder movement dysfunction gastritis burning stomach buy rabeprazole discount, the intervention enabled the client to progress faster in the transfer and gait training program than he would have had his left shoulder pain been attributed to angina. Risk factors and clinical presentation are discussed more completely in Chapter 17. Other risk factors include a blood clotting disorder,45 clavicle fracture,46 insertion of pacemaker wires, and arthroscopy of the shoulder or reconstructive shoulder arthroplasty. The therapist should be aware of the presence of any risk factors and watch for pain and pitting edema or swelling of the entire (usually upper) limb and/or an area of the limb that is 2 cm or more larger than the surrounding area indicating swelling requiring further investigation. Other symptoms include redness or warmth of the arm, dilated veins, or low-grade fever possibly accompanied by chills and malaise. Bruising or discoloration of the area or proximal to the thrombosis has been observed in some cases. Severe thromboses can cause superior vena cava syndrome; symptoms include edema of the face and arm, vertigo, and dyspnea. Most clients with endocarditis-related arthralgia have only one or two painful joints, although some may have pain in several joints. Pericarditis the inflammatory process accompanying pericarditis may result in an accumulation of fluid in the pericardial sac, preventing the heart from expanding fully. She works as a house painter and thinks the symptoms came on after a difficult job with high ceilings. She reports new symptoms of dizziness when getting up too fast from bed or from a chair. She is seeing a chiropractor and a naturopathic physician for a previous back injury 2 years ago when she fell off a ladder. She wants to try physical therapy because she has reached a "plateau" with her chiropractic care. Past Medical History: Other significant past medical history includes a total hysterectomy 4 years ago for unexplained heavy menstrual bleeding. She does not smoke or use tobacco products but admits smoking marijuana occasionally and being a "social drinker" (wine coolers and beer on the weekends or at barbeques). Physical therapy intervention can be initiated, but must be reevaluated on an ongoing basis. Eliminating the TrPs, improving her posture, and restoring full shoulder and neck motion will aid in the differential diagnosis. True postural hypotension must be accompanied by both blood pressure and pulse rate changes. Depending on the results, medical evaluation may be warranted, especially if no underlying cause can be found for the dizziness. Although there is no reported change in her vision or loss of balance with the dizziness, a vestibular screening examination is warranted. Given her age and risk factors, she should be asked when her last physical examination was done. If she has not been seen since her hysterectomy or within the last 12 months, she should be advised to see her personal physician for follow-up. If baseline bone density studies have not been done, then she should pursue this now. Likewise, she should ask her doctor about baseline testing for thyroid, glucose, and lipid values if these are not already available. In a primary care practice, risk factor assessment is a key factor in knowing when to carry out a screening evaluation. In any practice, we must know what effect a medical condition can have on the neuromuscular and musculoskeletal systems and watch for any links between the visceral and somatic systems. Because of its location in the posterior upper abdominal cavity in the retroperitoneal space and touching the diaphragm, the upper urinary tract can refer pain to the (ipsilateral) shoulder on the same side as the involved kidney. The scoring provides a tool to use in determining the need for additional testing. Information transmitted by renal and ureteral pain receptors is relayed by sympathetic nerves that enter the spinal cord at T10 to L1; therefore, renal and ureteral pain is typically felt in the posterior subcostal and costovertebral regions (flank). The distention or stretching of the renal capsule, pelvis, or collecting system from intrarenal fluid accumulation. Ischemia of renal tissue caused by blockage of blood flow to the kidneys can produce either a constant dull or sharp pain. True renal pain is seldom affected by change in position or movements of the shoulder or spine. If the diaphragm becomes irritated because of pressure from a renal lesion, ipsilateral shoulder pain can be the only symptom or may occur in conjunction with other pain and associated signs and symptoms. For example, generalized abdominal pain may develop accompanied by nausea, vomiting, and impaired intestinal motility (progressing to intestinal paralysis) when pain is acute and severe. Nerve fibers from the renal plexus are also in direct communication with the spermatic plexus, and because of this close relationship, testicular pain may also accompany renal pain in males. Shoulder pain that is not affected by movement or provocation tests requires a closer look. The presence of constitutional symptoms, constant pain (even if dull), and failure to change the symptoms with a position change will also alert the therapist to the need for a more thorough screening examination. A past medical history of cancer is always an important risk factor requiring careful assessment. This is true even when patients/clients have a known or traumatic cause for their symptoms.
For example gastritis diet 8i cheap 10 mg rabeprazole mastercard, contraction, guarding, and splinting of the rectus abdominis and muscles above the umbilicus can occur with dysfunction of the stomach, gallbladder, liver, pylorus, or respiratory diaphragm. Impairment of the ileum, jejunum, appendix, cecum, colon, and rectum are more likely to result in muscle spasm of the rectus abdominis below the umbilicus. The clinical picture is one that is easily confused with the primary pathology of the spinal segment. Dysphagia Dysphagia (difficulty swallowing) is the sensation of food catching or sticking in the esophagus. This sensation may occur (initially) just with coarse, dry foods and may eventually progress to include anything swallowed, even thin liquids and saliva. Dysphagia may be caused by achalasia, a process by which the circular and longitudinal muscular fibers of the lower esophageal sphincter fail to relax, producing an esophageal obstruction. Certain8 types of drugs, including antidepressants, antihypertensives, and asthma drugs9 can make swallowing difficult. After going through the questions, it may be helpful to leave the conversation open. Perhaps leave the client with this thought: · If you do not know the answer right now or if you just have not noticed, please feel free to let me and your physician know if you notice any changes. Odynophagia Odynophagia, or pain during swallowing, can be caused by esophagitis or esophageal spasm. To differentiate esophagitis from coronary ischemia: upright positioning relieves esophagitis pain, whereas cardiac pain is relieved by nitroglycerin or by supine positioning. Bleeding may not be obvious; serial hemoccult tests and laboratory tests (checking for anemia and iron deficiency) are needed. Diarrhea and ulcerative colitis are discussed in greater depth separately in this chapter. Bright red blood usually represents pathology close to the rectum or anus and may be an indication of rectal fissures. Melena, or black, tarry stool, occurs as a result of large quantities of blood in the stool. When asked about changes in bowel function, clients may describe black, tarry stools that have an unusual, noxious odor. The odor is caused by the presence of blood, and the black color arises as the digestive acids in the bowel oxidize red blood cells. It may be necessary to ask about bowel smears on the undergarments or difficulty getting wiped clean after a bowel movement. The following series may guide the therapist in this area: Esophageal varices are dilated blood vessels, usually secondary to alcoholic cirrhosis of the liver. Blood that would normally be pumped back to the heart must bypass the damaged liver. Bleeding from internal or external hemorrhoids (enlarged veins inside or outside the rectum), rectal fissures, or colorectal carcinoma can cause bright red blood in the stools. Rectal bleeding from anal lesions or fissures can occur in individuals who engage in anal sexual intercourse. Clients who have received pelvic radiation for gynecologic, rectal, or prostate cancers have an increased risk for radiation proctitis, which can cause subsequent (delayed) rectal bleeding episodes. Epigastric Pain with Radiation Epigastric pain perceived as intense or sharp pain behind the breastbone with radiation to the back may occur secondary to long-standing ulcers. For example, the client may be aware of an ulcer but does not relate the back pain to the ulcer. Anyone with epigastric pain accompanied by a burning sensation that begins at the xiphoid process and radiates up toward the neck and throat may be experiencing heartburn. A screening interview and evaluation is especially helpful when clients have not sought medical treatment for a longstanding problem. For example, long-standing epigastric back pain will cause the individual to assume postures to reduce symptoms. If sustained for a long time, biomechanical changes in the spine can occur, potentially causing musculoskeletal dysfunction. A good medical history can be a valuable tool in revealing the actual cause of the back pain. Back pain may be the overriding symptom of obstipation, especially in older adults who do not have regular bowel movements or who cannot remember if their last bowel movement was several weeks ago (Case Example 8. Keep in mind the individual who has low back pain with constipation could also be manifesting symptoms of pelvic floor muscle overactivity or spasm. In such cases, pelvic floor assessment should be a part of the screening examination. Changes in bowel habit may be a response to many other factors such as diet (decreased fluid and bulk intake), smoking, side effects of medication (especially constipation associated with opioids), acute or chronic diseases of the digestive system, extra-abdominal diseases, personality, mood (depression), emotional stress, inactivity, prolonged bed rest, and lack of exercise (Table 8. Commonly implicated medications include narcotics, aluminum- or calcium-containing antacids. Transit time of the alimentary bolus from the mouth to the anus is influenced mainly by dietary fiber and is decreased with increased fiber intake. Additionally, motility can be decreased by emotional stress that has been correlated with personality. People with low back pain may develop constipation as a result of muscle guarding and splinting that causes reduced bowel motility. Pressure on sacral nerves from stored fecal content may cause an aching discomfort in the sacrum, buttocks, or thighs (Case Example 8.
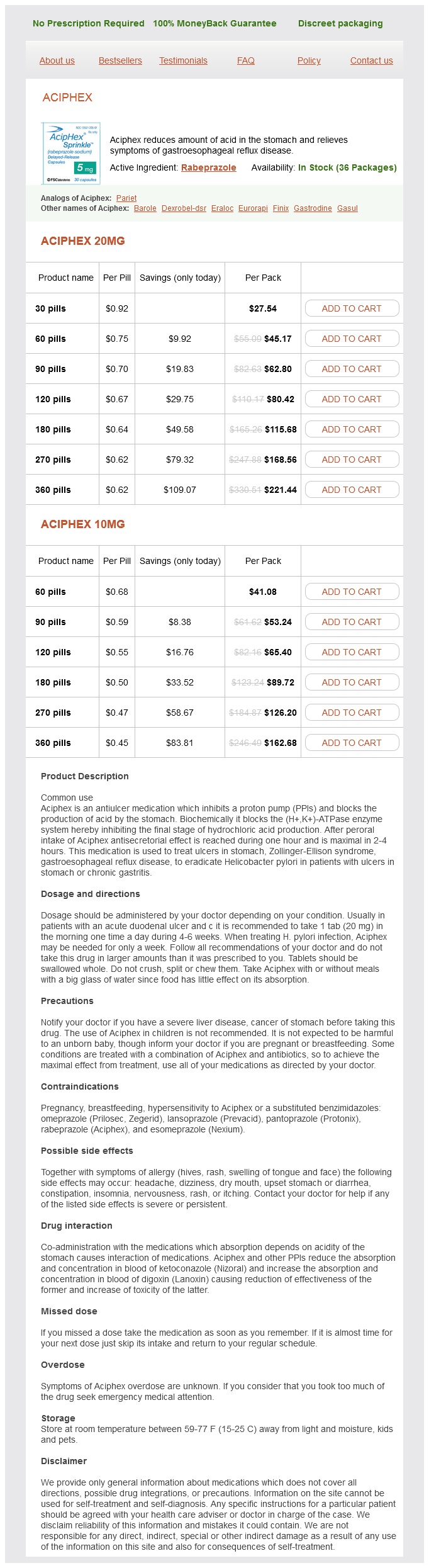
Rabeprazole Dosage and Price
Aciphex 20mg
- 30 pills - $27.54
- 60 pills - $45.17
- 90 pills - $62.80
- 120 pills - $80.42
- 180 pills - $115.68
- 270 pills - $168.56
- 360 pills - $221.44
Aciphex 10mg
- 60 pills - $41.08
- 90 pills - $53.24
- 120 pills - $65.40
- 180 pills - $89.72
- 270 pills - $126.20
- 360 pills - $162.68
Likewise viral gastritis symptoms order rabeprazole 20 mg, physical therapy intervention will not have any long-lasting effects unless the symptoms were caused by TrPs. The client had the usual childhood illnesses but had never broken any bones and denied use of tobacco, alcohol, or substances of any kind. Palpation of the upper chest, thorax, and ribs revealed pain during palpation of the right tenth rib (anterior). Knowing that transient osteoporosis can be associated with pregnancy,87-92 the therapist gave the client the Osteoporosis Screening Evaluation (see Appendix C-6 on). The client replied "yes" to three questions (Caucasian or Asian, mother diagnosed with osteoporosis, physically inactive), suggesting the possibility of rib fracture. Although the original x-ray film was read as negative, the physician ordered a different view (rib series) and identified a fracture of the tenth rib. The physician explained that the mechanical forces of the enlarging uterus on the ribs pull the lower ribs into a more horizontal position. Hepatic and Pancreatic Systems Epigastric pain or discomfort may occur in association with disorders of the liver, gallbladder, common bile duct, and pancreas, with referral of pain to the interscapular, subscapular, or middle/low back regions. Hepatic disorders may cause chest pain with radiation of pain to the shoulders and back. Cholecystitis (gallbladder inflammation) appears as discrete attacks of epigastric or right upper quadrant pain, usually associated with nausea, vomiting, and fever and chills. The pain has an abrupt onset, is either steady or intermittent, and is associated with tenderness to palpation in the right upper quadrant. A gallbladder problem can result in a sore tenth rib tip (right side anteriorly) as described in Chapter 9 (Case Example 17. Acute pancreatitis causes pain in the upper part of the abdomen that radiates to the back (usually anywhere from T10 to L2) and may spread out over the lower chest. When asked if any symptoms occur elsewhere in the body, the client may mention breast pain (Case Example 17. During examination of the upper quadrant, the therapist may observe suspicious or aberrant changes in the integument, breast, or surrounding soft tissues. Discharge from both nipples is more likely to be from a benign condition; discharge from one nipple can be a sign of a precancerous or malignant condition. Knowing possible causes of breast pain can help guide the therapist during the screening interview (see Table 17. She had recently moved here to be closer to her daughter, and no medical records have been transferred. At the end of the interview, when asked, "Is there anything else you think I should know about your health or current situation that we have not discussed Clinical Presentation: Examination revealed mild loss of strength in the left upper extremity accompanied by mild sensory and proprioceptive losses. The client had been aware of this pain, but she had attributed it to a separate medical problem. At the first follow-up visit, a letter was sent with the client that briefly summarized the initial objective findings, her progress to date, and the current concerns. She returned for an additional week of physical therapy to complete the home program for her shoulder. A medical evaluation ruled out breast disease, but medical treatment (medication) was indicated to address cardiovascular issues. A complete evaluation with advanced imaging may be needed to uncover the true underlying etiology as in the reported case of fibular pain in a patient with a history of breast cancer that turned out to be an incomplete nondisplaced distal fibular stress fracture with no evidence of tumor or mass (Case Example 17. A previous history of cancer is always cause to question the client further regarding the onset and pattern of current symptoms. This is especially true when a woman with a previous history of breast cancer or cancer of the reproductive system appears with shoulder, chest, hip, or sacroiliac pain of unknown cause. The client gave a month-old history of an ankle sprain while running; symptoms were made worse by running and there were no advanced imaging studies to rule out cancer metastases. Standard radiographs of the ankle were read as normal by the radiologist, but the therapist was suspicious of an observed irregularity in the distal fibula. Although it is more typical in women, both men and women can have chest, back, scapular, and shoulder pain referred by a pathologic condition of the breast. Clinical Presentation For the most part, breast pain (mastalgia), tenderness, and swelling are the result of monthly hormone fluctuations. Cyclical pain may become worse during perimenopause when hormone levels change erratically. It is unpredictable and may be constant or intermittent, affecting one or both breasts in a small area or the entire breast. The pain may continue along the medial aspect of the ipsilateral arm to the fourth and fifth digits, mimicking pain of the ulnar nerve distribution. Jarring or movement of the breasts and movement of the arms may aggravate this pain pattern. Pain in the upper inner arm may arise from outer quadrant breast tumors, but pain in the local chest wall may point to any pathologic condition of the breast. Nipple discharge in women is common, especially in pregnant or lactating women, and does not always signal a serious underlying condition. Injury, hormonal imbalance, underactive thyroid, infection or abscess, or a tumor are just a few possible causes of nipple discharge. Mastodynia Mastodynia (irritation of the upper dorsal intercostal nerve) that causes chest pain is almost always associated with ovulatory cycles, especially premenstrually. The presentation is usually unilateral breast or chest pain and occurs initially at the premenstrual period, and later, more persistently throughout the menstrual cycle. Mastitis Mastitis is an inflammatory condition associated with lactation (breastfeeding).
© 2025 Adrive Pharma, All Rights Reserved..