General Information about Nolvadex
In conclusion, Nolvadex (Tamoxifen) is a highly effective and generally prescribed medicine for the therapy and prevention of breast most cancers in ladies. By blocking the results of estrogen on breast cancer cells, Nolvadex helps to reduce the chance of recurrence and lowers the prospect of developing breast most cancers in high-risk individuals. While it may have some potential unwanted effects, the benefits of Nolvadex far outweigh the risks. If you or a beloved one has been recognized with breast cancer, converse to a physician about whether or not Nolvadex is the best therapy choice. Remember, early detection and therapy can save lives.
Nolvadex is often taken in pill kind and is often prescribed for a interval of five to 10 years, relying on the individual case. It is important to take Nolvadex precisely as prescribed by a doctor, as it works greatest when taken constantly.
Breast most cancers affects millions of ladies worldwide and is a quantity one explanation for demise for girls. However, there could be hope within the form of Nolvadex (Tamoxifen), a medication that's commonly used to treat breast most cancers in women. In this text, we are going to take a better have a glance at this medicine, its uses, and how it works to struggle breast most cancers.
In addition to treating breast most cancers, Nolvadex has been shown to scale back the danger of growing breast cancer in high-risk girls. This is as a outcome of it has the ability to block estrogen receptors within the breast tissue, lowering the amount of estrogen available to stimulate the expansion of cancer cells.
In uncommon instances, Nolvadex has been related to an elevated threat of uterine most cancers. However, this risk is low, and regular check-ups with a health care provider can help detect any potential problems early on.
While Nolvadex is usually nicely tolerated, it does have some potential unwanted aspect effects. The commonest unwanted effects include hot flashes, vaginal discharge, irregular menstrual durations, and mood swings. Some ladies may also experience blood clots, which is normally a severe aspect effect. It is necessary to debate any issues or unwanted facet effects with a physician.
Nolvadex is usually prescribed for ladies who've been recognized with early-stage breast most cancers, as it's efficient in stopping the recurrence of breast most cancers after surgical procedure, chemotherapy or radiation therapy. It can be utilized in girls who've a high risk of developing breast most cancers, both as a outcome of a household history of the disease or as a result of they've sure genetic mutations, such because the BRCA1 or BRCA2 gene.
Nolvadex is a medicine that's used to treat breast most cancers that's hormone receptor optimistic, that means that the most cancers cells have receptors for the hormones estrogen and progesterone. These hormones can stimulate the expansion of cancer cells, and Nolvadex works by blocking the results of these hormones on breast most cancers cells.
Nolvadex is a selective estrogen receptor modulator, which implies it has a singular capacity to bind to estrogen receptors and block the results of estrogen in sure tissues, whereas having estrogen-like results in other tissues. In the case of breast cancer, Nolvadex binds to estrogen receptors on breast cancer cells, stopping estrogen from stimulating their progress.
The therapist palpates either the lumbar interspinous spaces or the pelvic girdle to ensure that neutral is maintained (no rotation occurs) as the knee is slowly taken laterally (abduction and external rotation of the hip) the women's health big book of exercises free download nolvadex 10 mg buy low cost. Lifting the weight of the leg off the floor and lowering the leg into a fully extended position are high-level tasks, especially in those patients with muscular legs. Also, supine, or crook lying, progressions are high level for patients with pelvic girdle disability and/ or pain as this is the most challenging position to control the pelvis. In these cases, tasks in more upright positions such as sitting and supported standing can be added to the program before the higher progressions of leg loading in supine are achieved (Chapter 12). Should the femoral head lose its centered position relative to the acetabulum, the patient is not ready to progress to leg dissociation tasks at this time. Only the femur should move during this task; the lumbar spine and pelvis should remain in neutral. The task can be progressed by having the patient maintain the lift of the top knee and then lift the foot of the same leg (increase the lever arm). Clinically, the therapist would palpate the joint/ segment of poor control noted in the assessment of this task to ensure an optimal strategy was chosen and trained. A further progression would be to have the patient extend the abducted/externally rotated hip from this position. The leg should then flex, the ankles should approximate, and the knee then lowers to return to the starting position. It is important to teach the patient what it feels like when they lose control so that the task can be monitored and progressed at home. Remind the patient to use the load effort task analysis during the practice to ensure they are using an optimal strategy. Check for excessive bracing or rigidity of the rib cage (rib cage wiggle) and monitor lateral costal expansion breathing. Pillows or towels under the abdomen or thorax can be used to obtain the correct alignment. Ask the patient to bend one knee to 90 flexion, lifting the foot and then lowering it to the table. Once sagittal plane motion is controlled, introduce a rotation challenge by having the patient (C) externally and (D) internally rotate the femur. The task can be progressed by having the patient: (a) externally rotate the hip while maintaining intrapelvic control and a centered femoral head. When a cue is given that results in a contraction of psoas, which is isolated from the superficial hip flexors and adductors, most patients with failed load transfer through the hip are able to perform trunk and leg dissociation tasks with an optimal strategy (centered femoral head). This is not to say that other, deeper, muscles such the obturators or gemelli do not co-contract; this is still a matter of speculation. The key point is to ensure that the resultant strategy keeps the femoral head centered and allows the hip to move in the desired direction(s). A common best position for this is crook lying with feet supported over a bolster or with one foot. Palpate psoas with one hand and the dominant superficial hip muscles with the other. If the best neutral position is sidelying or prone, palpate the femoral head with one hand and the dominant superficial hip muscles with the other. Teach the patient how to palpate either psoas or the femoral head in the chosen neutral position. In this illustration, the patient is palpating the anterior groin while the therapist palpates tensor fascia latae, rectus femoris, and sartorius laterally. Several verbal cues are tried (see text) and the load effort task analysis is used to confirm the best cue/strategy for optimal recruitment of the hip flexors. In this example the therapist is palpating TrA bilaterally to monitor the activation of the deep muscle system during the task. As the leg moves into the outer range, the superficial hip flexors will activate to some degree, but this activity should not result in rigidity of the hip joint. The load effort task analysis will confirm whether the cue chosen facilitates a better strategy for loading through the hip in that reduced effort will be required to move the leg with the best cue. Connect along this wire thinking of gently compressing the femur into the hip socket. Connect along this wire thinking of gently suspending the vertebra after connecting the hip. The lumbopelvis should remain in the neutral position, the femoral head should remain centered, and a difference in effort to perform this task should be noted by both the patient and the therapist. Ankle plantarflexion (heel lift) can be used as an assist to get the foot off the wall. Palpate the lumbopelvis and the femoral head and ensure the strategy is optimal for maintaining a neutral lumbopelvis and centered femoral head. The task is progressed by moving the patient farther away from the wall, thus increasing the level arm. Finally, the task is performed over the edge of a table so that the foot can be lowered past the level of the table and the hip can move into full extension. Initially the patient will only be able to move the leg through a small range of motion. It is important to teach the patient what it feels like when they lose control (load effort task analysis) so that the task can be monitored and progressed at home. Be sure to check for rigidity of the rib cage and hip, and to monitor lateral costal expansion breathing to prevent excessive activation of the superficial muscles. Lifting the weight of the leg off the floor and lowering the leg into a fully extended position are high level, especially in those patients with muscular legs. In these cases, tasks in more upright positions such as sitting and supported standing can be added to the program (Chapter 12) before the higher progressions of leg loading in supine are achieved.
There should be a symmetrical amount of lateral movement with only a small amount of force menopause belly generic nolvadex 20 mg amex. A loss of this lateral joint play is an indication of a restriction of movement and overactivation of the superficial muscle system. General principles for coordinating the deep and superficial muscle systems (Box 11. If there is excessive superficial muscle activity, there will be a non-optimal pattern of rib cage expansion, bilaterally or unilaterally. Often there is minimal lateral costal expansion and excessive upper rib cage expansion). The movements should be slow and controlled in both the concentric and eccentric phases of movement. Two types of task can be used: those that control dissociation of the arm from the trunk, and those that control dissociation of the leg from the trunk. This practice builds on the foundation laid during training for coactivation of the deep muscle system and is preparatory for the next stage of rehabilitation building new strategies for meaningful tasks, function, and performance (Chapter 12). Often only one progression is used while simultaneously training more total body strategies (Chapter 12). A general guideline is to use the base position (sidelying, prone, supine, or crook lying) in which the patient was most successful at achieving the chord cue, and then use arm or leg movements/loading to add a further challenge. Palpation of the poorly controlled joints noted during the assessment will reveal whether or not control is maintained throughout the task. Observation of the orientation between the pelvis and the rib cage will reveal whether or not an optimal strategy for activation of the superficial muscle system is occurring. Adding verbal cues/images for the superficial Aim for high repetitions to build endurance (massed practice is an essential component for rewiring neural networks). Start with only as many repetitions as the patient can perform with an effective deep and superficial muscle system activation and control of the movement (sometimes as few as three to five repetitions), and progress to three sets of 10 repetitions with 2 minutes of rest between sets. Ensure that the deep muscle system does not turn off and that there are no signs of loss of control (previously found in the assessment). The therapist palpates for the recruitment and tonic contraction of the transversus abdominis while providing gentle pressure on the sternum to cue maintenance of the thoracic kyphosis and to prevent loss of neutral into thoracolumbar extension. Palpate transversus abdominis and multifidus at the dysfunctional level(s), ensuring that recruitment occurs with this cue. The shoulders should not flex or extend; movement occurs only at the elbow joints. The patient will require adequate length in the latissimus dorsi muscles to perform this progression with good control of the lumbar lordosis. Palpate the dysfunctional area (lumbar spine, sacroiliac joints) to ensure no loss of control of the neutral position. Hand weights can be added to increase the challenge to the spine while concurrently strengthening the arm muscles. Trunk and leg dissociation crook lying Several authors have described various leg loading tasks and their progressions (Hall & Brody 1999, Richardson et al 1999, Sahrmann 2001). Should the femoral head lose its centered position relative to the acetabulum during any of these tasks, the patient is not ready to progress to leg dissociation at this time. Palpate the segment(s) of poor control to ensure that no rotation occurs in the lumbar spine or pelvis. This phase of the task challenges extension and rotation control; the return of the leg back to the flexed position challenges flexion and rotation control. The easiest position from which to start the slide is the crook lying position; to increase the challenge have the patient start the slide with the leg straight. The task can also be changed from a single leg slide to alternating slides (from moving one leg at a time to moving both legs at the same time, one sliding down while the other slides up). Careful observation and palpation of the femoral head is necessary to ensure that the patient is not butt-gripping and pushing the femoral head anteriorly. The patient initially cues their release, align, and connect images for the deep muscle system and then flexes their hips to 90 such that the knees are vertically over the hip joints. The task can be progressed by having the patient extend the knee as the foot is lowered (increase the lever arm). When to refer for prolotherapy Prolotherapy (Cusi et al 2010, Dorman 1994, 1997) is indicated when there has been a loss of integrity of the articular system restraints (articular system impairment) and the neural and myofascial systems cannot provide sufficient compression to compensate and control the joint under load. When the myofascial and neural systems are functioning well, co-contraction of the muscles of the deep system should compress the joint, increase its stiffness, and reduce the neutral zone of motion to zero. If the 365 Trunk and leg dissociation hip joint control progressions Patient position. Cue the image that facilitates a co-contraction of the deep muscle system of the the Pelvic Girdle healthy myofascial and neural systems are unable to control motion in the neutral zone, it is unlikely that conservative treatment will be successful; this is the primary indication for prolotherapy (Video). Fibroblasts then migrate into the inflamed tissue and produce collagen, which increases the stiffness of the capsule/ligament. Typically, the capsule/ligaments are injected every 26 weeks, and the treatment is repeated for three to six sessions. The role of the therapist during this process is to ensure that the joint is supported with an external support or tape to prevent excessive shearing of the joint and to ensure that optimal alignment is maintained. As prolotherapy is often painful, the therapist should be prepared to provide emotional support during this process. Once the myofascial and neural systems can affect the neutral zone of motion (the joint glide can be reduced with a cocontraction of the deep muscle system), recovery of the articular system restraints has reached a point where appropriate motor control and movement training can now be implemented.
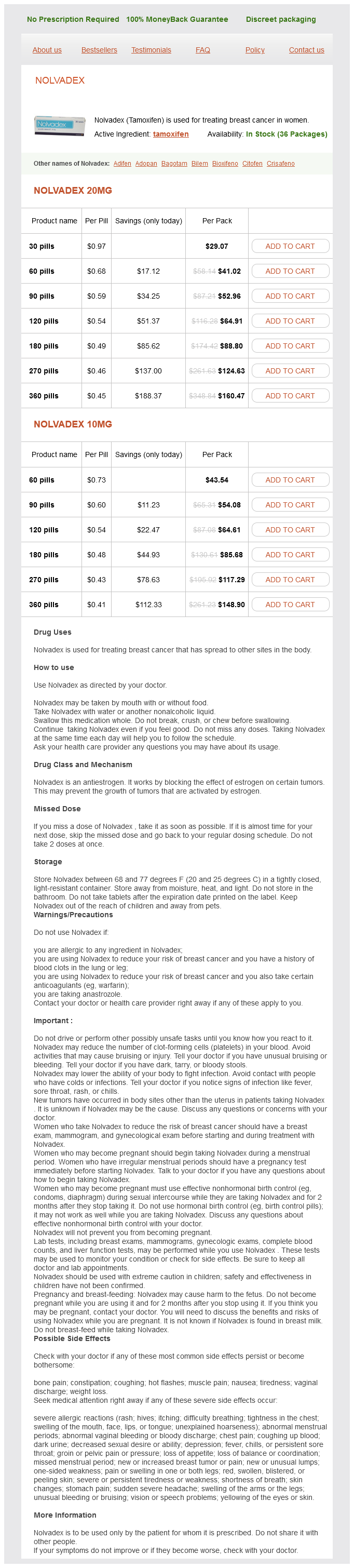
Nolvadex Dosage and Price
Nolvadex 20mg
- 30 pills - $29.07
- 60 pills - $41.02
- 90 pills - $52.96
- 120 pills - $64.91
- 180 pills - $88.80
- 270 pills - $124.63
- 360 pills - $160.47
Nolvadex 10mg
- 60 pills - $43.54
- 90 pills - $54.08
- 120 pills - $64.61
- 180 pills - $85.68
- 270 pills - $117.29
- 360 pills - $148.90
The talus should remain centered on the top of the calcaneus and the loss of talar position during the transference of weight suggests that a more detailed assessment of the foot is in order menopause back pain discount nolvadex 10 mg online. The innominate should remain posteriorly rotated relative to the ipsilateral sacrum throughout the task. Note the timing of any loss of control (loss of femoral head centering) during this task (early, middle, late); 3. The two bones should move as a unit as the pelvic girdle tilts anteriorly over the weight bearing lower extremity. Watch and feel for early, middle, or late anterior rotation of the innominate relative to the sacrum. Remember that the amplitude of motion for the sacroiliac joint is very small in weight bearing (46) and even when the pelvis unlocks completely during this task the movement is very subtle, yet palpable. If a segmental hinge or buckle is present, note the timing of this in relation to any femoral head displacement. Often the low back gives way when the hips fail to move and it is not uncommon for B. If in the standing postural examination one femoral head is noted to be anterior, particular attention is paid to the response of this hip during movement tasks. If the femoral head fails to center, note whether this induces a rotation of the pelvis as a consequence or causes the pelvic joints to unlock or lose control. The patient palpates the manubriosternal junction and the pubic symphysis as a reference point for thoracopelvic orientation during the squat. As a back-gripper, this is difficult for this model to simulate; note the persistent posterior tilt of the upper thorax. The interspinous spaces between the lower lumbar vertebrae are palpated with one hand and the intersegmental mobility noted and compared between levels as the patient squats. If a segmental hinge into flexion or extension is felt (one segment flexes or extends excessively compared to those above and/or below it), the timing of this non-optimal motion should be assessed (early, middle, or late). It is common to find excessive motion segmentally in the lumbar spine when one or both hip joints fail to move optimally into flexion during a squat. If unlocking of one side of the pelvis has already been determined (by palpating the innominate and sacrum. Also note the timing of the loss of lumbar segmental control relative to pelvic girdle unlocking. Use verbal and manual cues to correct the biomechanics of one region and observe the impact of this correction on the others (see case report Louise,). Step forward/step backward Step forward/step backward task analysis is integral to walking and running and thus to many sports as well. The patient has been given cues to relax the back muscles to allow the thorax to gently tilt anteriorly (not to purposely anteriorly tilt the thorax but rather to relax the muscles that are causing the posterior tilt). This provides some indication of how committed she is to this strategy for squatting. Cues to relax the posterior muscles of the deep buttock (let the sitz bones go wide) and allow the femurs to center in the acetabulum are given and the response noted. She was, and still is, a dancer and back-gripping is a common strategy among this group. Note the timing (early, middle, or late) of any loss of control (unlocking) during the task; 2. Note the timing of any loss of control (loss of femoral head centering) during this task (early, middle, late). Note the ability of the femur to rotate externally and internally while the patient holds a squat. When the strategy for this task is optimal, loads will be transferred without creating articular rigidity. As such, the hip and foot should be free to move even though they are bearing weight. Rotation and sidebending should occur as the pelvis rotates in the transverse plane; however, these movements should be evenly distributed througout the lumbar curvature. If a segmental hinge or buckle is present, note the timing of this in relationship to any unlocking of the pelvic girdle, femoral head displacement, or lack of mobility. Often the low back gives way when the hips fail to move, or as a consequence of the loss of control of the pelvic girdle under the lumbar spine;. Note the ability of the pelvis to tilt laterally to the left and right while the patient maintains a squat position. This task reveals the ability of the hip abductors and adductors to contract eccentrically and concentrically, and many hip imbalances can be seen and felt during this task. In this illustration, the therapist is palpating the adductors during a left lateral tilt of the pelvis to ensure they are able to lengthen eccentrically during this task. Non-optimal vectors of force (vector analysis) are easily palpated during this task. Non-optimal foot, ankle, knee, and thorax biomechanics can be extrinsic drivers of failed load transfer in the pelvis and their contribution may become more evident in these tasks. Counter-rotation between the lower thorax and the pelvis is 197 the Pelvic Girdle A. While the patient maintains the squat position, ask them to rise up onto their toes bilaterally.
© 2025 Adrive Pharma, All Rights Reserved..