General Information about Nitroglycerin
People with sure medical situations, similar to a historical past of low blood pressure or head injuries, should use nitroglycerin with warning. It may also interact with different medications, similar to erectile dysfunction medicine and certain antibiotics, so it is essential to inform your doctor about all the medicines you take.
Nitroglycerin is primarily used to prevent angina assaults, but it can additionally be used to deal with ongoing chest pain. It is usually prescribed to sufferers with coronary artery illness, a condition by which the arteries that provide blood to the guts become narrowed. This causes inadequate blood move and oxygen to the guts, resulting in angina. Nitroglycerin can be used earlier than physical actions which will trigger angina, corresponding to train or sexual exercise.
In addition to treating angina, nitroglycerin has different makes use of as well. It is usually used in emergency conditions, corresponding to a coronary heart attack, to alleviate chest ache and improve blood move to the center. It can also be used within the therapy of hypertension, coronary heart failure, and other heart-related situations.
Nitroglycerin is out there in numerous types, including tablets, sprays, ointments, and patches. The pill type is the most generally used and is positioned beneath the tongue for quick absorption into the bloodstream. The spray kind is sprayed onto or beneath the tongue, whereas the ointment is applied to the chest space. The patch type is placed on the skin and delivers a gradual amount of the medication over a period of time.
Nitroglycerin, also recognized as glyceryl trinitrate, was first discovered in 1847 by Italian chemist Ascanio Sobrero. However, it wasn't till 1879 that its potential as a coronary heart treatment was acknowledged by William Murrell, a British doctor. He found that nitroglycerin may relieve chest pain and improve blood flow to the guts.
Nitroglycerin is a powerful medication generally used to treat chest pain. It is primarily used to forestall episodes of angina, a type of chest ache that happens due to decreased or restricted blood circulate to the center. This treatment belongs to a class of medicine often known as nitrates and has been a mainstay within the treatment of cardiovascular illnesses for over a century.
Since then, nitroglycerin has been broadly used for the administration of angina in patients with coronary heart disease. It works by enjoyable and widening the blood vessels, permitting extra blood and oxygen to circulate to the guts, and decreasing the workload on the heart. This results in a lower in chest pain and discomfort.
In conclusion, nitroglycerin is a vital treatment for the management of continual chest ache attributable to coronary heart disease. Its capacity to alleviate ache and enhance blood circulate to the guts has made it a important part in the therapy of angina. However, it could be very important use this medication underneath the guidance of a healthcare skilled and to listen to its potential unwanted facet effects. With proper utilization, nitroglycerin can provide much-needed aid to these affected by heart illness.
As with any treatment, nitroglycerin could trigger unwanted facet effects in some individuals. Common side effects include headaches, dizziness, hypotension (low blood pressure), and flushing. In rare cases, it could cause a extreme drop in blood strain, leading to fainting or even a coronary heart assault. It is necessary to hunt medical consideration if any of those unwanted facet effects occur.
Risks and Complications Potential complications include infection acne natural treatment nitroglycerin 6.5 mg buy amex, hemorrhage, potential reaction to the medications instilled including anaphylaxis, neurovascular damage, pneumothorax, intravascular 181 Spine Anatomy and Injections: Thoracic Spine injection, subdural puncture, spinal cord injury, and the potential that the procedure may not be effective. A chest radiograph is not routinely necessary unless the patient reports symptoms suggestive of pneumothorax. Vital signs and neurological function are assessed and documented before discharge. However, it causes just as much morbidity, and additionally can affect respiratory effort, resulting in respiratory compromise. Patients may present with associated radiculopathy, degenerative disk disease, spondylosis, stenosis, scoliosis, rib fractures, tumors, or after undergoing thoracic surgery. Anatomically, intervertebral discs, dura, fascia, muscles, ligaments, or the facet joints are all capable of generating pain in the mid and upper back. Therapeutic injections may include either local anesthetics for pain relief or corticosteroids for anti-inflammatory effects. In a review of therapeutic, fluoroscopically guided thoracic transforaminal injections, 12 adverse postinjection effects were noted in 296 injections, for a total complication rate of 4. All but one event were considered minor and included local numbness, muscle spasm, vasovagal response, headache, or lightheadedness. Pneumothorax occurred once, but according to the authors "could have been avoided. By comparison, a review of 2,217 selective lumbar blocks demonstrated a minor complication rate of 5. Computed tomography may provide resolution and trajectory guidance to minimize these complication and ensure that the pleural space is not entered. Under new reimbursement guidelines, all imaging has been bundled with the respective procedures and these differences are mitigated. Reports have demonstrated that these procedures can be performed safely in less than 10 minutes, comparable to use of fluoroscopic guidance. Conscious sedation is rarely indicated unless the patient is extremely anxious, which usually can be resolved with discussion prior to procedure reassuring the patient of minimal discomfort with a 25-gauge needle and adequate local anesthetic. Excellent visualization of nerve root, facet joint, and lung as well as the spinal cord and dural sac is obtained. Computed tomography provides distinct advantages in performing thoracic nerve root injections, as it allows visualization of vasculature in the vicinity of the neuroforamen. However, for thoracic facet intra-articular injections, the needle tip is placed into the posterior aspect of facet joint, while for thoracic facet medial branch block, the needle is placed at the junction between the facet joint and the transverse process. A preliminary report of a randomized double-blind, active controlled trial of fluoroscopic thoracic interlaminar epidural injections in managing chronic thoracic pain. Epidural steroid and clonidine for chronic intractable post-thoracotomy pain: a pilot study. Immediate complications and pain relief associated with 296 fluoroscopically guided thoracic foraminal nerve blocks. Influence of needle-tip position on the incidence of immediate complications in 2,217 selective lumbar nerve root blocks. Anatomy 15 Thoracic facets are directed more vertically than the lumbar facets, with the anterior segment of the joint located more cephalad. In the lower thoracic levels, usually at T11-T12 and T12-L1, the angle gradually transitions from a frontal to a sagittal orientation similar to the lumbar facets. The exception to this rule is that medial branches of C7 and C8 may travel caudally to levels as low as T3. They continue running medially and inferiorly across the posterior surface of the transverse process. The medial branches run medially, posteriorly, and inferiorly after they branch off the dorsal ramus, until they come in close relation with the superolateral corner of the transverse process. Diagnosis Diagnosis of thoracic facet joint arthopathy is attained through careful history taking and thorough physical examination. While diagnostic blocks are used to confirm the diagnosis, imaging studies are not usually required. The relation of the thoracic medial branches and the superolateral portion of the transverse process vary depending on their level. In the upper (A) and lower thoracic (C) levels, they come in contact with bone, while in midthoracic (B) levels, they do not come in contact with bone but instead are suspended in the intertransverse space. Pain extending into the midscapular region may come from either C7-T1-T2 or T2-T3. Pain from the T11-T12 z-joint generally extends into the paravertebral region around the site of injection out to around the iliac crest area. As with cervical and lumbar facets, paravertebral tenderness could be the best indicator of thoracic facet pain. Patients presenting with thoracic back pain should be thoroughly examined to rule out serious pathology. Facet-mediated pain is not associated with any signs of any neurological deficits (Box 15. Intervertebral thoracic disc displacement or herniation must be considered in the presence of radicular pain. Also, intrathoracic and intra-abdominal pathology that could explain the pain should be ruled out (Box 15. Intra-articular injections are technically more challenging in the thoracic region due to the steep, frontal orientation of the facet joints. As in the lumbar spine, the morphologic degeneration of thoracic facets seen in different imaging studies does not translate into painful and symptomatic joints. Costovertebral and costotransverse joints are synovial joints with nociceptive innervation, and may become symptomatic when they undergo degeneration.
If this is not modeled in the dish symptoms yeast infection order 6.5 mg nitroglycerin fast delivery, then the relevance to the human in vivo disease is, at best, very questionable. This is sort of a crucial question, since, as already mentioned, the field does not have much else to fall back upon. The answer is complex, and there are a range of issues to address, many actually never given much scrutiny by numerous investigators. First, needless to say, the various tests of validity need to be satisfied to a greater rather than lesser degree in in vivo models. The next best option is to use primates, but such experiments come with their own set of problems. Both problems lead to a justifiable reluctance by researchers to use primates in almost any experimental scenario. Another problem, one rarely addressed, is this: Primates are obtained for research either by capture or by breeding them in captivity. What this means for primate studies is that one can expect greater variability with a monkey population, especially in experimental treatments involving any form of drug, than with a colony rodent population. The solution to this problem is to increase numbers, as is done in human drug trials, but this then runs into the previously mentioned problem of cost. The results seemed to suggest that there were no significant impacts of the vaccines on the neurobehavioral development or any structural features of the injected monkeys. The problem lay in the nature of the model in comparison to the epidemiology of the human disease. Thus, to correctly model a wild-type human population with a wild-type monkey population, the researchers should have used vastly more monkeys in each treatment group. No doubt they had done a proper power analysis to calculate the number of animals needed, but the very fact that it was a wild-type population made this otherwise very reasonable effort problematic in terms of the final interpretation. If such problems attend the use of primates, what about more common experimental species, such as mice and rats These have the advantage that they are less likely to suffer from wild-type population issues, but this becomes a problem in its own right as they are not likely to be representative of humans in two regards. First, they are far removed in the mammalian family tree from primates and can exhibit quite different biochemical and metabolic processes, not only from humans, but from each other (see. Second, while amongst humans individual genetic variations in expression can be quite different (as can variations in living conditions, types of food, conditions of water, etc. The problem that arises is that these issues are typically not dealt with in the design of experiments, at least in most mammalian studies. One solution to issues of variability in neurological disease studies is to increase the levels of the putative causal factor, be it genetic or molecular. Similarly, toxin studies often employ much higher concentrations of the suspected substances than most human neurological disease victims would likely be exposed to . And yet the widespread near consensus, at least that voiced publicly, is that while the models may not be "perfect," they are the best that the field has. The "best we have" is a pretty thin basis for understanding disease mechanisms, let alone designing effective, targeted therapeutic interventions for human patients. This last point is perhaps crucial for understanding why apparently successful animal studies almost never turn into successful outcomes in human trials. One recent report in the literature illustrates why such a disconnection in so-called "translational" medicine may arise. These outcomes have been critiqued, mostly on methodological grounds (Cauwels et al. While the Seok study specifically dealt with gene expression following various kinds of trauma, there is no reason to suppose the same general outcomes. As already mentioned, while a number of investigators acknowledged the potential problems posed by the Seok study, the response in the neurological disease literature was distinctly muted. K-means clustering of 4918 genes responsive to human systemic inflammation over time. Perhaps most researchers who did note the Seok and Burns studies did not want to believe them. And, in the absence of acting on the issue, perhaps by seeking other models, scientific and professional inertia might instead lead to rationalizations and the 164 Neural Dynamics of Neurological Disease continued use of models that can be summarized as "not perfect, but the best we have. However, is not uncommon to find that male and female animals have been merged in in vivo studies, or, almost as often, that the sex of the animals in not mentioned at all. Other studies do acknowledge the potential for problems arising from this omission, but given the realities of cost and the logistics of having large numbers of animals, some investigators sensitive to the potential problems posed by animal sex solve them by studying either males or females alone. Given the differential expression of human neurological diseases in human males and females, the picture that emerges from in vivo studies that report only the results of one sex is, at best, incomplete. The studies that merge the two sexes, in contrast, are likely to generate frankly misleading outcomes. If an experimenter uses a mouse neuron to model a similar type of human neuron, say a motor neuron in the spinal cord, the time frame of the different phases of synaptic transmission between axon and muscle is going to be broadly very similar. Indeed, it will generally be true across most mammalian species, other vertebrates, and in some cases even invertebrates. However, it is only an assumption, and likely not a very good one, that the same will apply across different ages of mice and humans. Given this, few researchers would try to model a 1-month-old human spinal motor neuron by looking at a 1-month-old mouse motor neuron. In spite of this, researchers routinely assume that one can model age-related neurological disease conditions in various model systems regardless of their age in relation to humans presenting the disease. While this might be true proportional to overall lifespan, it is almost certainly not true in terms of the various biochemical processes that necessarily occur over time.
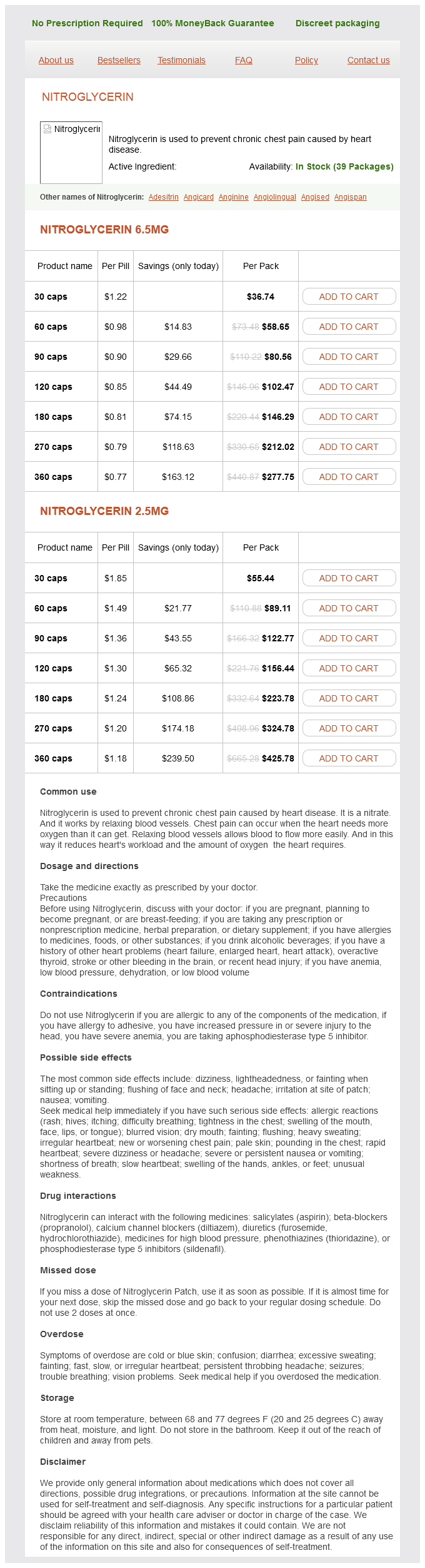
Nitroglycerin Dosage and Price
Nitroglycerin 6.5mg
- 30 caps - $36.74
- 60 caps - $58.65
- 90 caps - $80.56
- 120 caps - $102.47
- 180 caps - $146.29
- 270 caps - $212.02
- 360 caps - $277.75
Nitroglycerin 2.5mg
- 30 caps - $55.44
- 60 caps - $89.11
- 90 caps - $122.77
- 120 caps - $156.44
- 180 caps - $223.78
- 270 caps - $324.78
- 360 caps - $425.78
This outcome suggested that genetic factors were not causal in most cases medicine vial caps purchase nitroglycerin with paypal, the exception being for the early-onset forms of the disease. In addition, a genome screen for sibling pairs suggested a genetic linkage on chromosomes 1, 9, 10, and 16 for the sporadic form of the disease as well (DeStefano et al. This strategy arises from the view 2 Clinical and Economic Features of Neurological Diseases 27 that this loss is the crucial and perhaps initial feature of the disease in human patients. A number of genetic models using transgenic animals expressing various mutant proteins have also been created and tested. Notable examples are some of those neurological disease variants already mentioned. In population terms, this is comparable to the United States, which has a roughly 10 times larger population. This is only one state amongst 50, so the accuracy of these data are not certain for the United States overall. In Canada, the data do not seem to be reliable, although one report for the province of Manitoba showed no increase from 1980 to 2006 (Lix et al. Nursing home care will be a major contributor to medical costs and reduced employment will be a major indirect cost (Kowal et al. Its formal debut was given in 1865 by Jean Martin Charcot, a French neurologist (Charcot, 1865). These features also eventually occur when disease onset begins in the spinal cord and spreads rostrally. The upper motor neurons controlling voluntary movement are those arising from the motor cortex or brain stem 30 Neural Dynamics of Neurological Disease which carry motor information by way of spinal tracts to the lower motor neurons. These upper motor neurons are the large pyramidal cells (termed "Betz cells") found in layer V of the primary motor cortex. Lower motor neurons are found in the gray matter of the spinal cord (termed "anterior horn cells"), in the anterior nerve roots, or within the cranial nerve nuclei in the brain stem. These others include primary lateral sclerosis, which affects upper motor neurons alone, and progressive muscular atrophy, which affects only lower motor neurons. The former innervate the extrafusal muscle fibers of skeletal muscles to initiate muscle contractions. Another main pathology involves shrunken anterior nerve roots (Yachnis and Riviera-Zengotita, 2014), likely a consequence of motor neuron loss. Evidence for increased astrocytic and microglial proliferation suggests inflammatory processes during the disease time course. This conclusion remains controversial and appears to strongly depend on the antibody being used to label the misfolded protein (Liu et al. El Escorial was designed to aid in diagnosing and classifying patients for clinical studies, therapeutic trials, and molecular genetics research. However, the sensitivity of the criteria has been found to be low in clinical practice and early diagnosis (Traynor et al. In 2006, clinical researchers proposed a modification to the existing criteria to increase sensitivity without losing specificity (de Carvalho et al. The modified criteria have been shown to significantly increase sensitivity, resulting in earlier diagnosis and thus earlier potential entry into clinical drug trials (Douglass et al. For example, it is easy to perform and can be used to measure progression and predicted survival times (Czaplinski et al. Although the loss of motor function leading to death definitely involves the motor neuron cell bodies, their axons, and the muscles they innervate, it is not yet clear which of these might be the initial locus of degeneration. One view holds that the motor neurons are the proximal site of the disease and thus are primarily affected. In this view, as the motor neurons degenerate, their axons and eventually the neuromuscular junction degenerate as well, to be followed by muscle atrophy. The correct sequence is not known in human patients and it seems likely there is considerable variation. A series of papers by various investigators, mostly from Japan, have described a change in collagen that occurs coincidentally with the loss of motor neurons (Ono et al. The fact that both neurons and skin are of ectodermal origin may be an important clue to disease origin, although this point has not been widely investigated. This observation suggests an environmental etiology, rather than one of genetic origin. As cited previously, the generation of transgenic mice carrying various copies of the mutant human gene has been a key focus of animal studies of the disease since the early 1990s. Other mutations are constantly being discovered, as will be described in Chapter 5. It shows up neuropathologically as deposits of tau protein in the frontal cortex (Irwin et al. In a paper published in 1906, Alzheimer described the characteristic behavioral features of the disease, including the selective loss of memory and the inability to learn new tasks (Alzheimer, 1906). It also involves neurons that make the neurotransmitter acetylcholine in the nucleus basalis of Meynert. Altogether, dementias of all types represent the most common form of intellectual impairment in those over 60 years of age. Dementia can be the consequence of stroke, head trauma, alcoholism, drug intoxication, infectious diseases of the brain, or exposure to toxic molecules such as aluminum (see Chapter 6). In fact, the only definitive diagnosis of the disease is made following post-mortem histological examination of the brain. Each of these cases could fall into an emerging disease categorization of "tauopathies," in which the proposed underlying theme is a crucial involvement of abnormal tau (Bayer, 2015).
© 2025 Adrive Pharma, All Rights Reserved..