General Information about Lisinopril
Apart from its primary use for hypertension, Lisinopril has also been discovered to be beneficial in other conditions such as coronary heart failure, diabetic kidney disease, and prevention of heart attacks in patients with a history of cardiovascular disease. This is why it's not uncommon for doctors to prescribe Lisinopril to sufferers with these situations.
In conclusion, Lisinopril is an effective medication for treating hypertension and has been shown to considerably lower the chance of heart illness and stroke. However, it should not be seen as an various to a healthy life-style. A balanced food plan, regular train, and stress management strategies should also be included within the management of hypertension. Remember, prevention is always better than treatment, and early detection and treatment of hypertension can save lives.
Lisinopril is usually considered secure for use in most people, but there are some precautions to bear in mind. Individuals with a history of angioedema (swelling of the face, lips, tongue, or throat) should not take Lisinopril. It is also not recommended for pregnant ladies, as it might hurt the fetus. Therefore, it is essential to inform your doctor of any medical situations or drugs you take earlier than starting Lisinopril.
If left untreated, high blood pressure can result in serious well being issues, including coronary heart illness, kidney illness, and stroke. This is why it is necessary to monitor and handle blood pressure levels via lifestyle adjustments and, if essential, medication corresponding to Lisinopril.
Lisinopril is a medication commonly prescribed for the treatment of high blood pressure or hypertension in adults and youngsters over the age of 6. It is a half of a category of medicine generally known as angiotensin-converting enzyme (ACE) inhibitors, which work by stress-free blood vessels, allowing blood to move more easily and reducing blood strain.
Hypertension is a situation in which the force of blood towards the walls of the arteries is persistently too excessive, putting a pressure on the center and growing the risk of coronary heart attack or stroke. It is estimated that over 1 billion folks worldwide have hypertension, making it one of the most common continual circumstances. Despite its prevalence, many individuals are unaware that they've hypertension, because it typically presents with no signs. This is why it is sometimes called the “silent killer”.
Lisinopril has been proven to effectively lower blood strain, with studies displaying that it can scale back blood stress by a mean of 11/6 mm Hg. This discount in blood stress not solely decreases the chance of coronary heart attack and stroke but additionally reduces the strain on the center, making it easier for it to pump blood around the physique.
The medicine comes in pill type and is usually taken as soon as a day, with or with out food. The dosage might vary depending on the individual’s age, medical historical past, and response to treatment. It is essential to follow the prescribed dosage and to not cease taking the treatment with out consulting a physician, as suddenly stopping might trigger a sudden increase in blood strain.
As with any medicine, Lisinopril may cause unwanted effects in some individuals. The most common unwanted effects embody a dry cough, dizziness, headache, and fatigue. In rare circumstances, extra serious unwanted facet effects such as severe allergic reactions, kidney problems, and liver problems might happen. It is important to seek medical consideration if any of these symptoms happen.
Lisinopril works by inhibiting the activity of the enzyme ACE, which is responsible for the production of a hormone called angiotensin II. This hormone causes blood vessels to slim and constriction of blood circulate, leading to increased blood pressure. By blocking the production of angiotensin II, Lisinopril helps blood vessels relax and widen, permitting blood to move more simply and decreasing blood strain.
Higher levels of silica exposure can lead to accelerated silicosis with a latency period of 510 years blood pressure chart too low order lisinopril with a mastercard, and very high levels of exposure can lead to acute silicoproteinosis within a few months (4,24). As a result, the latency period can vary from as short as 2 months to as long as 40 years, and the disease History and examination 333 Table 19. Constitutional symptoms do occur and cough is frequently the initial pulmonary symptom. Laboratory testing may be helpful to assess occupational exposure to asbestos if an occupational history is difficult to obtain (28). Briefly, mononuclear cells are isolated and cultured with and without beryllium sulphate. These criteria for BeS provide a sensitivity of 88% and a specificity of 96% (27). Rapid growth of masses or development of cavitation should prompt a search for alternative or secondary diagnoses such as tuberculosis or lung cancer (1). Hilar lymphadenopathy is present in one-third of cases, but as with silicosis, to a lesser extent than in sarcoidosis. In advanced disease, honeycombing, conglomerate masses and emphysema can occur (1,27). Asbestosis: Early pathologic findings in asbestosis include peribronchiolar fibrosis that extends into the alveolar walls. The presence of asbestos bodies on biopsy supports a diagnosis of asbestosis but absence of asbestos bodies does not exclude asbestosis (29). Dark pigment dust with birefringent particles may be present in the center of the nodules (1). For deconditioned patients, pulmonary rehabilitation can improve quality of life (1). This recommendation is based on the doseresponse relationship of lung injury described for asbestosis and silicosis, with higher levels of cumulative exposure leading to worsening lung injury (4,5). For other agents, despite the lack of strong evidence, removal from the exposure is still advisable (1). For patients with more significant respiratory impairment or severe symptoms or evidence of progressive decline in lung function, oral corticosteroids are considered first-line agents. Observational studies suggest that treatment with glucocorticoids leads to improved pulmonary function, radiographic abnormalities, symptoms and functional status. A steroid-sparing agent can be considered for those with significant side effects related to glucocorticoids. Patients with silicosis who are diagnosed with active tuberculosis should receive therapy for 8 months rather than the standard of 6 months to reduce the risk of recurrence (1,34). Higher levels of cumulative exposure and advanced disease at diagnosis are risk factors for progression (29,35). Silicosis similarly progresses slowly, taking an average of 12 years for end-stage fibrosis to develop in one study. Indium tin oxide has recently been described in workers in the flat-panel display industry, primarily in Asia. Exposed workers may develop pulmonary alveolar proteinosis and fibrotic interstitial lung disease (36). For example, denim sandblasting emerged as a new risk factor for silicosis in Turkey (37). A number of treatments have been tried without convincing success in silicosis, and possible cell-based therapy has been proposed (44). Comparison of registries of interstitial lung diseases in three European countries. Asbestos and other fiberrelated diseases of the lungs and pleura: Distribution and determinants in exposed populations. The principle of the sentinel health event and its application to the occupational diseases. Interstitial lung disease induced by exogenous agents: Factors governing susceptibility. Prevalence and incidence of benign asbestos pleural effusion in a working population. Exposure and mineralogical correlates of pulmonary fibrosis in chrysotile asbestos workers. Machining risk of beryllium disease and sensitization with median exposures below 2 µg/m3. Emphysema in silicosis: A comparison of smokers with nonsmokers using pulmonary function testing and computed tomography. An official American Thoracic Society statement: Diagnosis and management of beryllium sensitivity and chronic beryllium disease. The comparison of high-resolution computed tomography findings in asbestosis and idiopathic pulmonary fibrosis. The alveolar haemorrhage syndromes and pulmonary vasculitides are a complex group of potentially life-threatening conditions that require a thoughtful diagnostic approach and often require emergent therapeutic interventions. This article details the clinical approach to the diagnosis and management of these syndromes with a focus on clinically relevant pearls of wisdom. We advocate for a collaborative approach to these complex diseases and consideration of early referral to a tertiary care centre. Anaemia or haemoptysis are common but may not always be identified at the time of presentation.
The results from large clinical trials albeit the good safety profiles have demonstrated divergent findings in cardiac function in patients with myocardial infarction [49e55] arteria jugularis discount lisinopril 2.5 mg with amex. Different methods have been employed to deliver stem cells to the damaged myocardium. The most frequent are intracoronary and intramyocardial approaches with diverse advantages and disadvantages for each one (Table 3. Most of the studies have used intracoronary delivery as preferred administration route [49]. Cells are delivered over the lumen of an inflated over the wire balloon catheter placed in the reopened coronary artery after percutaneous coronary intervention [56]. The direct delivery to the infarcted myocardium and the relatively low invasiveness are the main advantages. Direct intramyocardial injection of cells has also been used, especially in models of chronic ischaemic cardiomyopathy, and facilitates cell delivery despite the potential arrhythmiogenic effects, and the need for concomitant open heart surgery [57]. Most of the studies have resulted in beneficial outcomes for the cardiac function. Furthermore, this improvement was coupled with a concomitant decrease in infarct size and an increase in the left ventricle viable mass, implying the robust regeneration of myocardial tissue. Despite the favorable results observed in some individuals treated with stem cells, certain clinical expectations were not achieved because the levels of improvement in cardiac tissue structure or functionality were less than those previously observed in experimental trials [66]. Beyond these landmark studies, there are more than 20 smaller trials in the field of stem Stem-Cell Therapy 329 cell transplantation currently published. Albeit several challenges, such as optimization of the therapeutic protocols and technological improvement of stem cell delivery devices, it is believed that the current ongoing studies will accelerate the further development and acceptance of stem cell therapy and the optimal selection of stem cell type. Clinical trials have shown only a modest or negligible improvement of cardiac function [39]. First, the rather small number and the selection of patients, and their preparation have to be considered. Second, factors related to the cell administration, such as the injection of an insufficient number of cells, the biodistribution of injected cells, the use of wrong cell type, the extent of cellular differentiation of these cells within the target area, the use of an inappropriate delivery method, or possible inappropriate timing relative to the age of the infarct [67]. Despite all efforts, the specific cell types conferring therapeutic effects have not been yet defined [68,69]. Intense debate is focused on definition of specific markers of endothelial and other vascular progenitor cells. Moreover, differences between animal models and humans, including the absence of comorbidities in the animal model, should be considered [39]. Last, results of chronic postinfraction studies are less supportive for stem cell therapy than acute myocardial infarction studies. Compared to chronic disease, several trials in acute phase of myocardial infarction found that cell treatment significantly improved left ventricular function [71]. Damaged myocardium can regenerate from the stem cells that enter the cell cycle, contributing to changes in the myocardial mass. Early animal studies reported very promising results for stem cell therapy, with robust remasculinization. However, despite intensive research, the principal mechanisms have not yet been fully elucidated. Moreover, there is an ongoing debate in the field of basic stem cell research as to which cell type is more suitable. This lack of knowledge translates into the currently available clinical trials, which were only partially able to reproduce the groundbreaking findings from animal studies. There is a need to put even more efforts in order to clarify the principal regenerative properties of different stem cells and to develop promising approaches for their clinical application. It is important to emphasize in specific patient-related factors that may have an impact on cell therapy outcomes, such as severity of atherosclerosis or cardiovascular risk factors. Although cell therapy holds therapeutic promise for clinical applicability, further clinical trials powered to detect differences in mortality and to identify the most beneficial approaches are warranted in order conclude whether stem cell transplantation will eventually join the standard therapeutic armamentarium and improve both the mortality rate and quality of life. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Genetically selected cardiomyocytes from differentiating embronic stem cells form stable intracardiac grafts. Transplantation of human embryonic stem cell-derived cardiomyocytes improves myocardial performance in infarcted rat hearts. Human embryonic stem cells can differentiate into myocytes with structural and functional properties of cardiomyocytes. Cardiac stem cells: isolation, expansion and experimental use for myocardial regeneration. Myocardial regeneration by activation of multipotent cardiac stem cells in ischemic heart failure. Cardiac stem cells delivered intravascularly traverse the vessel barrier, regenerate infarcted myocardium, and improve cardiac function. The relative potency and safety of endothelial progenitor cells and unselected mononuclear cells for recovery from myocardial infarction and ischemia. Transdifferentiation of blood-derived human adult endothelial progenitor cells into functionally active cardiomyocytes. Cell therapy attenuates deleterious ventricular remodeling and improves cardiac performance after myocardial infarction. Factors affecting functional outcome after autologous skeletal myoblast transplantation. Autologous skeletal myoblasts transplanted to ischemia-damaged myocardium in humans. Autologous skeletal myoblast transplantation for severe postinfarction left ventricular dysfunction. Autologous intramyocardial injection of cultured skeletal muscle-derived stem cells in patients with non-acute myocardial infarction.
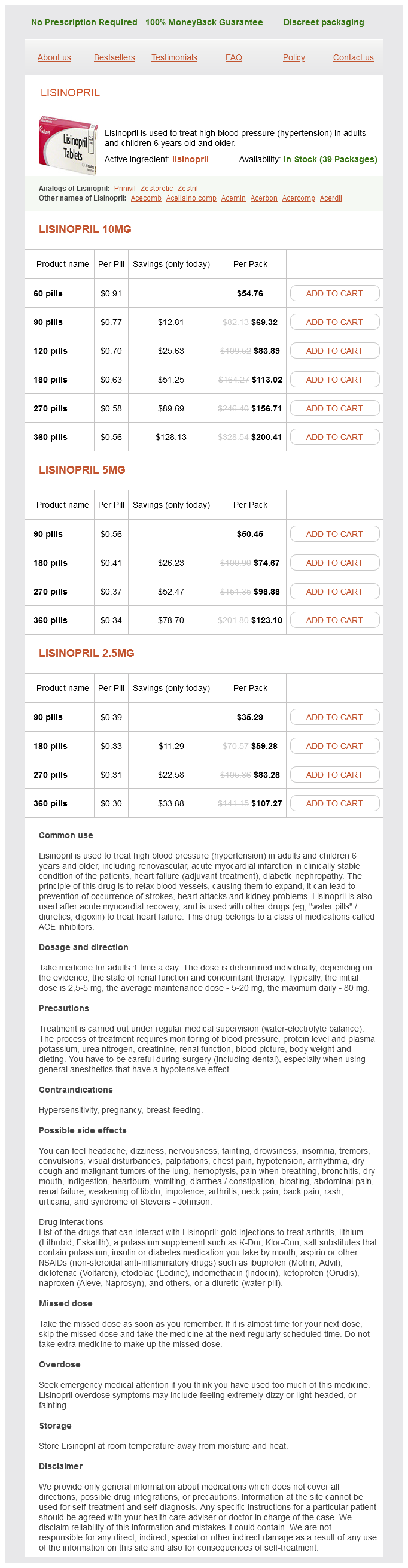
Lisinopril Dosage and Price
Lisinopril 10mg
- 60 pills - $54.76
- 90 pills - $69.32
- 120 pills - $83.89
- 180 pills - $113.02
- 270 pills - $156.71
- 360 pills - $200.41
Lisinopril 5mg
- 90 pills - $50.45
- 180 pills - $74.67
- 270 pills - $98.88
- 360 pills - $123.10
Lisinopril 2.5mg
- 90 pills - $35.29
- 180 pills - $59.28
- 270 pills - $83.28
- 360 pills - $107.27
As or all procedures that use contrast media arteria pulmonar discount lisinopril 5 mg without a prescription, emergency equipment should be readily available, and the technologist must be amiliar with the protocol in case o an allergic reaction by the patient. Patients who have known sensitivities may require premedication to minimize the risk. Common risks and complications include the ollowing: in at th p nct it: Bleeding usually can be con· Bl trolled by applying compression. I the axillary, brachial, or radial artery is used or catheterization, an additional risk may be damage to nearby nerves and arterial spasm. The ragment becomes an embolus; this causes great risk to the patient and is treated immediately. Neonates rom special care nurseries are covered with warming blankets during the procedure to maintain their body temperature. However, they should be given a thorough explanation o the procedure be ore signing the consent. However, angiographic procedures, especially cardiac catheterization, o ten are indicated to investigate congenital de ects. The patient remains on bed rest or a minimum o 4 hours, but the head o the bed or stretcher may be elevated approximately 30°. The a ected extremity is also checked or warmth, color, and numbness to ensure that circulation has not been disrupted. In addition, the angiographer is usually not required to compress the puncture site with the use o these closure devices. This technique is o ten e ective or patients who are taking anticoagulants, another added benef t. It is not unusual or geriatric patients to eel anxious be ore their procedure; they may ear alling o the narrow examination table. Reassurance and additional care rom the technologist throughout the procedure enable patients to eel secure and com ortable. A radiolucent mattress o additional padding on the examination table provides com ort to geriatric patients. Older patients may have tremors or di f culty holding steady; use o high mA results in shorter exposure times, which helps to reduce the risk or motion on the images. Angiography units may have specialized beam f ltration and pulsed uoroscopic capabilities to help ensure that the dose is kept to a minimum. Because scatter radiation largely contributes to sta dose, maximizing the distance between the sta member, the x-ray source, and the scattering object (the patient) is crucial. The distance between the image intensif er and the patient should be minimized, whereas the distance between the x-ray source and the patient should be maximized. In addition, using tools such as last image hold or the review o previously stored images may also assist in reducing dose to all. It is larger than conventional radiographic rooms and includes a sink and scrub area and a patient holding area. The room must have outlets or oxygen and suction, and emergency medical equipment must be nearby. The resultant image shows the structure as i it were completely f lled with contrast media. Subsequent uoroscopy shows the progress o the procedure over this re erence image. Alte rnative Mo dalitie s andPro ce dure s In addition to the specif c angiographic procedures described on subsequent pages, alternative modalities and procedures are available in clinical imaging centers or imaging the vascular system. T maintain o the ow rates necessary or angiography, an automatic electromechanical injector is used. The ow rate is a ected by many variables, such as the viscosity o the contrast media, the length and diameter o the catheter, and injection pressure. Depending on these variables and the vessel to be injected, the desired ow rate can be selected be ore injection. A ter the vessel o interest is catheterized under uoroscopic guidance, a small hand injection o contrast media is administered to ensure that the catheter is in an accurate position. For the imaging series, the electromechanical injector options are selected delivering a preset amount o contrast media. The rate o image acquisition is rapid, o ten in the range o several rames per second. Every injector is equipped with syringes, a heating device, a high-pressure mechanism, and a control panel. The heating device warms and maintains the contrast media at body temperature, reducing the viscosity o the media. In addition to sa ety, convenience, ease o use, and reliability o ow-rate settings, other eatures o an automatic mechanical injector include (1) ready light when armed and set or injection, (2) a slow or manual injector control to remove air bubbles rom the syringe, and (3) controls to prevent inadvertent injection or excessive pressure or volume injection. Nuclear medicine complements other imaging modalities because it provides primarily physiologic in ormation but little anatomic detail. Sonography may be used to image the patency o vessels and to demonstrate thrombus ormation, plaque, or stenosis. Color duplex (color ow Doppler) is also used in sonography to demonstrate the presence or absence o ow within a vessel, the direction o ow, and, with more sophisticated equipment, the velocity o ow. Echocardiography provides detailed images o the heart or investigation o numerous cardiac conditions, including valve disease, aneurysm, cardiomyopathy, myocardial in arction, and congenital de ects.
© 2025 Adrive Pharma, All Rights Reserved..