General Information about Lioresal
As talked about earlier, Lioresal works by appearing on the central nervous system, particularly the spinal wire. It enhances the consequences of a neurotransmitter referred to as GABA, which is liable for inhibiting the exercise of neurons within the mind and spinal twine. This results in a lower in nerve signals that cause muscle spasms, thereby offering relief to the affected muscular tissues.
Like any medicine, Lioresal might trigger unwanted side effects in some people. Common unwanted side effects embrace drowsiness, dizziness, weak spot, nausea, and complications. These side effects are usually gentle and may lower with continued use. More critical unwanted side effects, similar to problem respiratory, chest ache, and seizures, could occur in rare circumstances, and instant medical consideration should be sought if these symptoms are experienced.
Lioresal may also interact with different drugs, such as antidepressants and blood pressure drugs, so it's important to tell a healthcare skilled of all present medicines earlier than beginning Lioresal treatment. It shouldn't be taken with alcohol or other sedative drugs as this will increase the chance of sedation and drowsiness.
MS is a continual, progressive disease that impacts the central nervous system, causing a spread of symptoms together with muscle spasms, weakness, and numbness. These muscle spasms could be quite debilitating and might have an effect on a person’s capacity to perform every day duties and actions. This is where Lioresal is obtainable in – it helps to relieve the symptoms of MS and enhance the quality of life for those dwelling with the situation.
Aside from treating muscle spasms, Lioresal has also been found to be useful in treating different signs associated with MS, such as ache, tremors, and bladder or bowel issues. It can additionally be used in mixture with different drugs, corresponding to anti-inflammatory drugs, to additional enhance its efficacy.
Lioresal is a prescription medicine that is usually taken orally in the form of a pill or liquid. It can additionally be out there in an injectable type for many who have problem swallowing or have severe signs. The dosage of Lioresal may range depending on the severity of the signs and the individual’s response to the treatment. It is essential to comply with the dosage directions supplied by a healthcare skilled and to not cease or change the dosage with out consulting a physician.
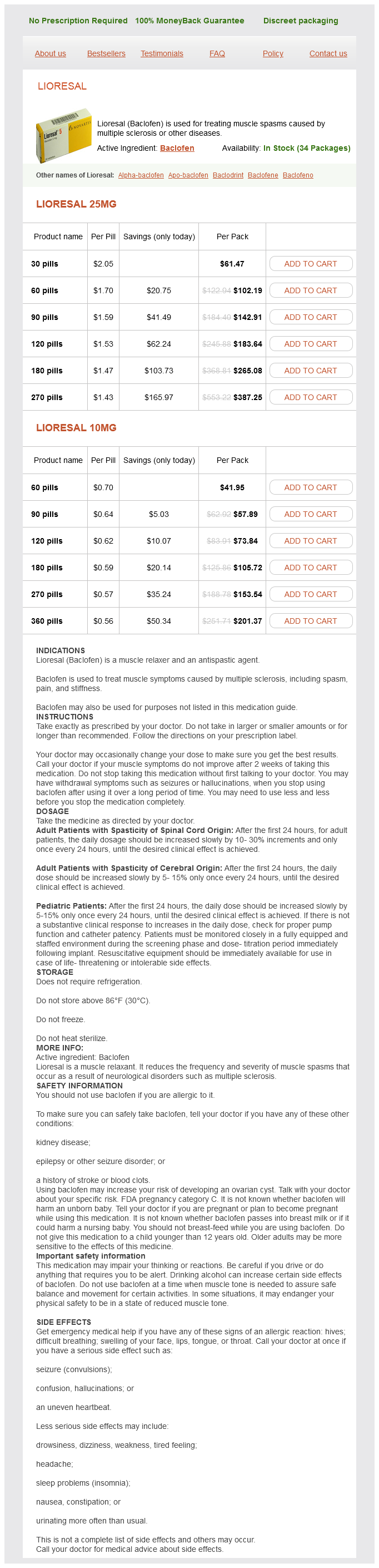
Lioresal, also recognized as Baclofen, is a drugs that's generally used to treat muscle spasms caused by multiple sclerosis (MS) and other neurological situations. It is a muscle relaxant that works by appearing on the central nervous system, particularly the spinal cord, to scale back the severity and frequency of muscle spasms.
The effectiveness of Lioresal in treating muscle spasms attributable to MS has been studied extensively, and it has been discovered to be extremely beneficial. It not solely helps to reduce back the frequency and depth of muscle spasms, but it additionally improves muscle stiffness and mobility. In addition to MS, Lioresal has additionally been used to treat muscle spasms attributable to different neurological conditions such as spinal cord injury, cerebral palsy, and stroke.
In conclusion, Lioresal is a extensively used medicine for the therapy of muscle spasms attributable to MS and different neurological conditions. It has been discovered to be extremely effective in lowering the severity and frequency of spasms, enhancing muscle stiffness and mobility, and offering relief to other associated signs. However, you will want to use Lioresal as prescribed by a doctor, be aware of potential unwanted facet effects, and notify a healthcare skilled of any current medicines to make sure safe and effective treatment.
It is characterized by hyperirritability back spasms 34 weeks pregnant cheap 10 mg lioresal, ever, and hard nonpitting edema that overlie the cortical hyperostosis. Pathologically, it involves the loss o periosteum with acute in ammatory involvement o the intratrabecular bone and the overlying so tissue. Similar symptoms may occur in iers when they suddenly ascend to high altitudes unprotected by counterpressure. It results rom the escape rom solution in the body uids o bubbles (mainly nitrogen) originally absorbed at higher pressure. Symptoms include headache; pain in the epigastrium, sinuses, and tooth sockets; itchy skin; vertigo; dyspnea; coughing; nausea; vomiting; and sometimes paralysis. There is a question o rupture o the round window membrane; hemotympanum and eustachian tube obstruction may occur. The syndrome is characterized by dwar sm, cranio acial anomalies, and bowing o the tibia and emur, with malormation o other bones. Respiratory distress is common, and the patient has an early demise in the rst ew months o li. In the otolaryngologic area, the patient exhibits a prominent orehead, at acies with a broad nasal bridge and low-set ears, cle palate, mandibular hypoplasia, and tracheobronchial malacia that contributes to the respiratory distress and neonatal death. Histologically, two temporal bone observations showed de ective endochondral ossi cation with no cartilage cells in the endochondral layer o the otic capsule. This syndrome is o en o unknown etiology, although some believe it is autosomal recessive. This syndrome is not to be con used with Pierre Robin syndrome, which presents with very similar clinical eatures. Cannon Nevus this an autosomal dominant disorder characterized by spongy white lesions o the oral and nasal mucosa. The lesions are asymptomatic and may be ound rom the newborn period with increasing severity until adolescence. Carotid Sinus Syndrome (Charcot-Weiss-Barber Syndrome) When the carotid sinus is abnormally sensitive, slight pressure on it causes a marked all in blood pressure due to vasodilation and cardiac slowing. It is also known as localized nodal hyperplasia, angiomatous lymph node hyperplasia, lymphoid hamartoma, and giant lymph nodal hyperplasia. Symptoms include tracheobronchial compression, such as cough, dyspnea, hemoptysis, or dysphagia. There are two histologic types: the hyaline vascular type and the plasma cell type. Follicles in the hyaline vascular type are traversed Cha pter 1: Syndromes and Eponyms 7 by radially oriented capillaries with plump endothelial cells and collagenous hyalinization surrounding the vessels. The ollicles in the plasma cell type are normal in size without capillary proli eration or hyalinization. It drains into the in erior petrosal sinus, which in turn drains into the internal jugular vein. The cavernous sinus syndrome is caused by thrombosis o the cavernous intracranial sinus, 80% o which is atal. The symptoms include orbital pain (V1) with venous congestion o the retina, lids, and conjunctiva. There is contralateral hemiplegia and diminished proprioception and tactile sensation. Champion-Cregah-Klein Syndrome this a amilial syndrome consisting o popliteal webbing, cle lip, cle palate, lower lip stula, syndactyly, onychodysplasia, and pes equinovarus. Chapple Syndrome this disorder is seen in the newborn with unilateral acial weakness or paralysis in conjunction with comparable weakness or paralysis o the contralateral vocal cord, the muscles o deglutition, or both. The disorder is secondary to lateral exion o the head in utero, which compresses the thyroid cartilage against the hyoid or cricoid cartilages or both, thereby injuring the recurrent or superior laryngeal nerve, or both. Charcot-Marie- ooth Disease this a hereditary and degenerative disease that includes the olivopontocerebellar, cerebelloparenchymal, and spinocerebellar disorders and the neuropathies. This disease is characterized by chronic degeneration o the peripheral nerves and roots; and distal muscle atrophy in eet, legs, and hands. It is also associated with hereditary cerebellar ataxia eatures, optic atrophy, and other cranial involvement. It involves heart de ects, breathing and swallowing di culties, hearing loss, vision loss, and balance problems. It is characterized by albinism, photophobia, nystagmus, hepatosplenomegaly, anomalous cellular granules, and development o lymphoma. Cle Lip Palate and Congenital Lip Fistulas this syndrome is transmitted in an autosomal dominant manner with 80% penetrance; it occurs in 1 per 100,000 live births. Usually bilateral, symmetrically located depressions are noted on the vermilion portion o the lower lip and communicate with the underlying minor salivary glands. The lip pits may be an isolated nding (33%) or be ound with cle lip palate (67% o cases). Associated anomalies o the extremities may include talipes equinovarus, syndactyly, and popliteal pterygia. Congenital lip pits have also been seen in association with the oral- acial-digital syndrome. Cockayne Syndrome Cockayne syndrome is autosomal recessive, progressive bilateral sensorineural hearing loss, associated with dwar sm, acial disharmony, microcephaly, mental de ciency, retinitis pigmentosa, optic atrophy, intracranial calci cation, and multiple dental caries. Patients succumb to respiratory or genitourinary in ection in the teens or twenties. Cogan Syndrome Nonsyphilitic interstitial keratitis and vestibuloauditory symptoms are characteristics o Cogan syndrome. Symptoms include episodic severe vertigo accompanied by tinnitus, spontaneous nystagmus, ataxia, and progressive sensorineural hearing loss.
Treatment Treat with the following: Steroid use is still not clearly beneficial muscle relaxant that starts with the letter z lioresal 25 mg with visa, although the best evidence for its efficacy is in elderly patients with severe pain. There is no benefit to routine subtyping of the specific strain of papillomavirus. Treatment Mechanical removal: this can involve cryotherapy with liquid nitrogen, laser removal, or trichloroacetic acid or podophyllin to melt them away. Resolution is slower; however, there is never any damage to the surround normal tissue and no pain. Primary Syphilis the chancre of primary syphilis is an ulceration with heaped-up indurated edges that is painless the majority of the time. In other words, these serologic tests need several weeks to become positive, and they are only 75 percent sensitive in primary syphilis. Both primary and secondary syphilis are treated with a single intramuscular dose of penicillin. In those patients allergic to penicillin, doxycycline orally for 2 weeks is the alternative therapy. Secondary Syphilis Secondary syphilis presents with a generalized copper-colored, maculopapular rash that is particularly intense on the palms and soles of the feet. The other manifestations of secondary syphilis are predominantly dermatologic as well: the mucous patch, alopecia areata, and condylomata lata. As above, both primary and secondary syphilis are treated with a single intramuscular dose of penicillin. Scabies and Pediculosis Scabies Scabies involves primarily the web spaces of the hands and feet but can also cause pruritic lesions around the penis and breast. Because Sarcoptes scabiei is quite small, all that can be seen with the naked eye are the burrows and excoriations around small pruritic vesicles. Lindane has equal efficacy but greater toxicity; thus, it is not the best initial therapy. Pediculosis (Lice and Crabs) Pediculosis tends to include the head and is easily transmitted by sharing hats and hairbrushes. Both organisms have an enormously high rate of transmission through sexual contact, with 90 percent transmission from a single contact. Diagnostic Testing Because pediculosis is caused by a much larger organism, scraping is not necessary. The organisms can readily be seen attached to hair-bearing areas, particularly under magnification. Lyme Disease More than 85 percent of patients who have Lyme disease develop a rash. The rash must be erythematous with central clearing and be at least 5 cm in diameter. This rash is so characteristic of Lyme that it is more important than serological testing in terms of confirming a diagnosis. If the rash is described, then go straight to therapy with oral doxycycline, amoxicillin, or cefuroxime. Nasal packing, retained sutures, or any other form of surgical material retained in the body can promote the growth of the type of Staph that produces the toxin. Diagnostic Testing Because there is no single specific test, cases are matters of definition. Treatment Vigorous fluid resuscitation Pressors, such as dopamine Antistaphylococcal medications, such as oxacillin, nafcillin, or cefazolin For methicillin- (oxacillin-) resistant strains, vancomycin or linezolid can be used. Anthrax Bacillus anthracis is usually a cutaneous infection acquired from contact with infected livestock. A papule appears that later becomes inflamed and develops central necrosis that is black in color; hence the name anthrax, which is the Greek word for "coal. Malignant and Premalignant Diseases Benign Lesions the predominant method of distinguishing between benign and malignant lesions is by the shape and color of the lesion. Benign lesions, such as the junctional or intradermal nevus, have the following characteristics: They do not grow in size. Melanoma these malignant lesions grow in size, have irregular borders, are uneven in shape, and have inconsistent coloring. Biopsy diagnosis is best performed with a full thickness sample, because tumor thickness is by far the most important prognostic factor. Seborrheic Keratosis this is a benign condition with hyperpigmented lesions occurring in the elderly with a "stuck on" appearance. Actinic Keratosis Actinic keratoses are precancerous lesions occurring on sun-exposed areas of the body in older persons. Therapy is universally with sunscreen to prevent their progression and recurrence. Squamous cell carcinoma develops on sun-exposed skin surfaces in elderly patients. It is particularly common on the lip, where the carcinogenic potential of tobacco is multiplicative. In this technique, instant frozen sections are done to determine when enough tissue has been removed to give a clean margin. A Koebner phenomenon is the development of lesions to the site of an epidermal injury.
Lioresal Dosage and Price
Lioresal 25mg
- 30 pills - $61.47
- 60 pills - $102.19
- 90 pills - $142.91
- 120 pills - $183.64
- 180 pills - $265.08
- 270 pills - $387.25
Lioresal 10mg
- 60 pills - $41.95
- 90 pills - $57.89
- 120 pills - $73.84
- 180 pills - $105.72
- 270 pills - $153.54
- 360 pills - $201.37
Anatomy · The acial nerve is a mixed nerve containing motor muscle relaxer sleep aid generic 25 mg lioresal otc, sensory, and parasympathetic bers. E erent motor bers rom the motor nucleus innervate the platysma, posterior belly o the digastric muscle, the stylohyoid muscle, the stapedius muscle, and the muscles o acial expression. The upper motor neuron tracts to the upper ace cross and re-cross be ore reaching the acial nerve nucleus in the pons, sending bilateral innervation to the upper ace. There ore, lesions proximal to the acial nerve nucleus spare the upper ace o the involved side, allowing orehead movement and eyelid closure, whereas distal lesions produce complete paralysis o the a ected side. E erent parasympathetic bers originating rom the superior salivatory nucleus are responsible or lacrimation and nasal secretions (via greater super cial petrosal nerve to lacrimal and nasal glands) and salivation (via chorda tympani nerve to submandibular and sublingual glands). A erent Components aste rom the anterior two-thirds o the tongue is transmitted by a erent bers to the nucleus tractus solitarius by way o the lingual nerve, the chorda tympani, and eventually the nervus intermedius, the sensory root o the acial nerve. The nerve runs anterior to the superior vestibular nerve and superior to the cochlear nerve. The allopian canal is narrowest within the labyrinthine segment, particularly at its entrance (meatal oramen). At the geniculate ganglion the nerve makes a 40° to 80° turn to proceed posteriorly across medial wall o the tympanic cavity, medial to the cochleari orm process, then above the oval window, and then under the lateral semicircular canal to the pyramidal eminence. The majority o intratemporal acial nerve injuries result rom trauma to the nerve in the tympanic and mastoid segments. Mastoid (vertical) segment: 10 to 14 mm, pyramidal process/second genu to stylomastoid oramen. T ree branches arise rom this segment: nerve to the stapedius muscle, chorda tympani nerve, and nerve rom auricular branch o the vagus nerve (Arnold nerve). A er emerging rom the stylomastoid oramen, the nerve courses anteriorly and slightly in eriorly, lateral to the styloid process and external carotid artery, to enter the posterior sur ace o the parotid gland. Once it enters the substance o the parotid gland, it bi urcates into an upper temporozygomatic division and a lower cervico acial division. The extensive network o anastomoses that develops between the various limbs is called the pes anserinus. Surgical Anatomy · Landmarks or identi cation o the extratemporal acial nerve: (a) Tragal pointer: nerve identi ed 1 to 1. The most common location o dehiscence, and also the most common site o iatrogenic injury during middle ear surgery, is the tympanic segment adjacent to the oval window. History · Any palsy demonstrating progression beyond 3 weeks or lack o any sign o recovery a er 6 months should be considered due to an underlying neoplasm until proven otherwise. Physical Examination · The initial evaluation should determine i the weakness is complete or partial. Remember that eyelid elevation is a unction o the levator palpebrae muscle, which is innervated by the oculomotor nerve, and will remain intact despite a total acial nerve paralysis. Central unilateral acial paralysis usually involves only the lower ace, as the innervation o the upper ace is derived rom bilateral upper acial motor neurons. In addition, the presence o emotional acial expression as well as lacrimation, taste, and salivation on the ipsilateral side suggest a central lesion. These unctions are not governed by the motor cortex o the precentral gyrus and, there ore would be una ected by lesions in these areas. Imaging Studies · The need or radiologic evaluation is based on the history and clinical course o each individual case. Gross Pa rt 2: Otology/Neurotology/Audiology Slight weakness noticeable on close inspection. Moderate dys unction Gross Obvious, but not dis guring di erence between the two sides. However, the presence and degree o enhancement have not been shown to correlate with the severity o paralysis, electrophysiologic test results, and prognosis or recovery. Electrophysiologic tests will reveal rapid and complete degeneration 72 hours a er injury. As long as the endoneurium is preserved, there will be complete recovery with return o normal unction. Characterized by wallerian degeneration, an unpredictable regeneration potential, and the likelihood o signi cant resultant dys unction and synkinesis. Results rom a single axon or a small group o axons innervating motor end units o numerous and separated muscles. Commonly used examples include the Schirmer test, the submandibular ow test, and the stapedial re ex test. These tests have been ound to correlate poorly with the site o injury and are unreliable in predicting recovery. While they are included in this discussion, they are rarely used in clinical practice today and indicated only i in ormation about a speci c unction is required. Functional recovery or incomplete acial paralysis is good and there ore prognostic testing is not required in when paralysis is incomplete. The electrodes are then placed in corresponding locations on the involved side, and the same procedure is per ormed. Cha pter 21: Fa cial Nerve Paralysis 373 · A suprathreshold electrical stimulus is used to elicit acial contraction on the normal and paralyzed side. Lacrimation (Schirmer Test) · Evaluates greater super cial petrosal nerve unction (ie, tear production). Stapedial Re ex · The stapedius muscle contracts re exively in both ears when one ear is stimulated with a loud tone. This alters the reactive compliance o the middle ear, which can be measured with impedance audiometry.
© 2025 Adrive Pharma, All Rights Reserved..