General Information about Lexapro
Depression is a psychological health disorder that affects approximately 6.7% of adults in the United States. It is characterised by feelings of unhappiness, hopelessness, and a loss of curiosity in activities that had been as soon as enjoyable. Some widespread symptoms embody changes in urge for food, bother sleeping or sleeping an excessive quantity of, problem concentrating, and thoughts of self-harm or suicide. In addition to therapy, antidepressants like Lexapro are sometimes prescribed to assist manage the symptoms of melancholy.
Lexapro can also be used to treat GAD, a situation that affects approximately 6.eight million adults in the united states GAD is characterised by excessive worry and pressure that is troublesome to regulate, and can intervene with every day life. People with GAD might expertise bodily signs similar to restlessness, fatigue, muscle rigidity, and difficulty sleeping. Like despair, therapy is often utilized in mixture with medicine to successfully manage GAD symptoms.
Lexapro, also called escitalopram, is a prescription medicine commonly used to deal with depression and generalized anxiousness disorder (GAD). It belongs to a category of antidepressants generally identified as selective serotonin reuptake inhibitors (SSRIs), which work by rising the degrees of serotonin within the mind. This helps to enhance temper, reduce nervousness, and general restore balance to 1's psychological health.
It is essential to note that like all antidepressants, there is a threat of worsening melancholy and ideas of self-harm or suicide when starting a brand new treatment. This is why it's essential to follow the dosage and frequency prescribed by a healthcare skilled and to speak any adjustments in signs to them. It can also be important to continue taking Lexapro as directed, even when symptoms enhance, to prevent a relapse.
In conclusion, Lexapro is a widely prescribed and effective medication for treating melancholy and GAD. Its capability to extend serotonin levels within the mind helps to enhance temper, cut back anxiousness, and restore stability to at least one's psychological well being. With its fewer unwanted aspect effects and approval to be used in youngsters and children, Lexapro is a valuable choice for these struggling with these situations. It is necessary to at all times consult with a healthcare professional before starting any new medicine and to communicate any changes in signs or considerations all through therapy.
Another advantage of Lexapro is that it has fewer unwanted effects in comparability with other kinds of antidepressants. Common side effects might include nausea, diarrhea, dizziness, and drowsiness, however these are often mild and temporary. Side effects are also much less likely to happen when taken consistently and at the prescribed dosage.
One of the important thing reasons why Lexapro is often prescribed for each depression and GAD is due to its similarity to the neurotransmitter serotonin. Serotonin is a chemical messenger in the mind that's answerable for regulating mood, sleep, and urge for food. In individuals with despair or GAD, there might be typically an imbalance in serotonin levels, which can contribute to their signs. Lexapro works by blocking the reuptake of serotonin, allowing more of it to remain in the mind and improve overall mood and mental well being.
In addition to being efficient in treating despair and GAD in adults, Lexapro can also be permitted to be used in youngsters and youngsters as younger as 12 years old for depression and 7 years old for GAD. It is important to observe youngsters and teenagers for any modifications in behavior or mood whereas taking Lexapro and to debate any issues with their physician.
If affected individuals (children) are undergoing surgery anxiety 504 plan lexapro 10mg for sale, an iliac crest biopsy can be evaluated, although admittedly this is performed with markedly less frequency than in the past, particularly while our molecular understanding has markedly increased. However, histomorphology studies done on these disorders have led to important insights on the pathogenesis of these disorders. On morphologic grounds, the chondro- dysplasias can be broadly classified into those disorders that (1) have a qualitative abnormality in endochondral ossification, (2) have abnormalities in cellular morphology, (3) have abnormalities in matrix morphology, and (4) in which the abnormality is primarily localized to the area of chondroosseous transformation. For example, in thanatophoric dysplasia, there is a defect in endochondral ossification with a very short, if almost hypertrophic, zone, a shortened proliferative zone, and overgrowth of the periosteum. In pseudoachondroplasia, there is a distinct lamellar pattern (alternating electron-dense and electron-lucent lamellae) in the rough endoplasmic reticulum of chondrocytes and a grossly abnormal matrix in diastrophic dysplasia, which leads to a characteristic ring around the chondrocytes. All of these findings are characteristic and diagnostic for these disorders and illustrates how morphology studies can play in integral part in the investigation of these disorders. Further, disorders across a phenotypic spectrum have been placed in bone families based on similar cartilage growth plate morphologic abnormalities. There has been significant progress in gene identification in these disorders, which has impact for affected individuals. As illustrated in Table 105-1, for those disorders in which the gene is identified, molecular diagnostic testing is potentially available. Molecular diagnosis can be used to confirm a clinical and radiographic diagnosis, predict carrier status in those families at risk for a recessive disorder, and, for some individuals, allow prenatal diagnosis of at-risk fetuses. With commercial availability of whole-exome sequence analysis, many high and low bone mass parallel sequencing panels are available, as well as whole-exome sequence analysis for rare disorders not available on panels. If there is no question regarding definitive diagnosis, then disease genes can be directly interrogated. Treatment the optimal management of this diverse set of disorders requires an understanding of their medical, skeletal, and psychosocial consequences. This is often best accomplished by centers that have a multidisciplinary approach, which include adult and pediatric physicians, as well as a group of physicians, geneticists, orthopedists, rheumatologists, otolaryngologists, neurologists, neurosurgeons, and ophthalmologists who are committed to the care of these patients. Most medical complications in these disorders result from orthopedic complications, and they vary depending on the specific disorder. This causes knee or ankle pain in many individuals, especially children, and consideration should be made for correction by osteotomies. Children and adults with skeletal dysplasias should have regular eye and hearing examinations because they are at increased risk for myopia, retinal degeneration, glaucoma, and hearing loss, depending on the disorder. Frequently, patients with these disorders have significant joint pain and, in some cases, joint limitations. Because most of these disorders result from mutations in genes critical to cartilage function, the cartilage at the joint surfaces may not provide adequate support and cushioning function. Last, weight control in adults with short stature is an ongoing issue and contributes to inactivity, loss of function, adult-onset diabetes, hypertension, and coronary disease. The majority of these individuals are of normal intelligence, have a normal life span, and lead independent and productive lives. The mean final height in achondroplasia is 130 cm for men and 125 cm for women, and specific growth charts have been developed to document and track linear growth, head circumference, and weight in these individuals. Clinically, these infants show central apnea, sleep apnea, profound hypotonia, motor delay, or excessive sweating. Other complications include upper airway obstruction, thoracolumbar kyphosis, and hydrocephalous in a small number of individuals. Craniofacial abnormalities lead to dental malocclusion, and appropriate treatment is necessary. As adults, the main potential medical complication is impingement of the spinal root canals, and this can be manifested by lower limb paresthesias, claudication, clonus, bladder, or bowel dysfunction. It is critical that these complaints are addressed because without appropriate decompression surgery, paralysis of the spinal cord can result. Biochemical and Molecular Abnormalities Based on clinical, radiographic, and histomorphologic similarities, skeletal dysplasias have been placed into bone dysplasia families. In recent years, there has been an explosion in our understanding of the basic biology of these disorders. This has resulted from advances in the human genome project that improved various methodology, including candidate gene approach, linkage analysis, positional cloning, human/mouse synteny, wholeexome and whole-genome analysis, allowing identification of the responsible disease genes (see Table 105-1). There are still skeletal dysplasias for which the disease-producing genes are unknown. Below are just some examples of the molecular mechanisms involved in the skeletal dysplasias. Both these disorders are associated with early-onset osteoarthritis, particularly of the hips and the knee, leading to joint replacements in many individuals in early adulthood. Mutations that result in a substitution for a triple-helical glycine residue appear to be the most common type of mutation. The explosion in delineating molecular defects has shown the complexity of cartilage as a tissue and the large number of cellular processes necessary for a normal skeleton. Because there is enormous clinical variability in these types, the subtypes will be discussed separately (Table 105-2). However, these disorders all share the same phenotypic finding of hypomineralization of the skeleton, although interesting bone quality is associated with overbrittleness. Individuals usually have mild short stature for their age or their unaffected family members, but are not as severe as seen in the other forms. The disorder is autosomal dominant, and in many cases, the individual is the first affected in their family. Other reported ocular defects include scleromalacia, keratoconus, and retinal hemorrhage. The enamel is normal, but the dentin is dysplastic; chipping of enamel occurs, and the teeth are subjected to erosion and breakage. During the second and third decades of life, a characteristic high-frequency sensorineural or mixed hearing loss can be detected.
Willingness from the surgeon depression zodiac order lexapro 10mg with mastercard, anesthesia, and nursing staff is essential for success of the bedside laparotomy. Complications after negative laparotomy for trauma: long-term follow-up in a health maintenance organization. Impact of increased use of laparoscopy on negative laparotomy rates after penetrating trauma. Open abdominal management after damage-control laparotomy for trauma: A prospective observational American Association for the Surgery of Trauma multicenter study. One hundred percent fascial approximation can be achieved in the post-injury open abdomen with a sequential closure protocol. It can be injured in isolation or involved with injury in either body cavity, and the most challenging concern is the identification of injury. Initially the injury may be asymptomatic with later development of herniation and strangulation of the stomach or other viscera. It is bounded above by both pleural spaces and the pericardium, which is attached to the central tendon. Structures immediately adjacent to the inferior side of the diaphragm include the liver, spleen, stomach, and to varying degrees the colon, omentum, and small bowel. The origin of the diaphragm includes the lower sternum, lower six costal cartilages and adjacent ribs, and medial and lateral lumbocostal arches. The insertion of the diaphragm is into the central tendon, an aponeurosis, located at the top of the dome, oriented transversely, and separated into three segments. At rest the diaphragm rises to the level of the fourth intercostal space on the right and the fifth intercostal space on the left. The aorta passes behind the diaphragm and between the crura where it has no attachments. Along with the aorta the thoracic duct and azygous vein pass through this opening. The esophagus traverses the esophageal hiatus mostly composed of the right crus along with the vagus nerves. The blood supply to the diaphragm is multiply redundant making necrosis extremely rare. Additional blood supply is from the superior phrenic, pericardiophrenic, musculophrenic, and the intercostal arteries. Lymphatic drainage is rich on both sides of the diaphragm with the peritoneal surface the major contributor to peritoneal lymphatic drainage. Innervation is principally through the phrenic nerves with some contribution of the sixth or seventh intercostal nerves to the costal region of the diaphragm. Both phrenic nerves enter the diaphragm near the anterior border of the central tendon. These nerves give branches along the thoracic surface of the diaphragm before penetrating it to spread branches in anterior, posterior, and lateral directions. The nerves are often buried deep in the muscle, and one should not rely on visualizing the nerves in order to choose incisions in the diaphragm. It participates in breathing, swallowing, coughing, defecation, emesis, micturition, parturition, sneezing, and vocalization. The displacement of abdominal viscera into the chest due to the pressure gradient between the abdomen and the chest may compromise both cardiac and respiratory function. Cardiac dysfunction due to reduced ventricular filling can lead to decreased cardiac output. Significant compression of the pulmonary parenchyma can lead to impaired ventilation on the ipsilateral side, and, if more severe, mediastinal shift and compression of the contralateral lung. As with any herniation of portions of the gastrointestinal tract, sequelae such as ischemia, necrosis, and perforation may develop. Unfortunately, there are no long-term outcome data that describe diaphragmatic function after repair for trauma. There are many reports of delayed repairs of diaphragmatic injuries, and this suggests that repair is durable and has little impact on either pulmonary or gastrointestinal tract function. Patients presenting in the obstructive phase often experience nausea, vomiting, early satiety, pain, dyspnea, postprandial pain, or generalized chest and abdominal pain. Patients may also present in extremis with signs and symptoms of septic shock due to ischemia or perforation related to strangulation or gangrene of incarcerated viscera or with cardiovascular collapse due to compression. In 2013, Zarour et al reviewed 773 patients with diaphragmatic injury and noted that 57% of injuries were on the left, 40% on the right and 3% were bilateral. Traumatic brain injury is present in half of the patients and is predictive of mortality. Intrathoracic injuries include pneumothorax, pulmonary contusion, lung lacerations, blunt myocardial injury, and aortic rupture. Specific intra-abdominal organs typically injured with penetrating diaphragmatic injury include the upper abdominal organs. Patients may have minimal signs of external injury or be experiencing severe shock and respiratory compromise that may or may not be directly related to the diaphragmatic injury. In the less severely injured, possible signs and symptoms include shoulder pain, epigastric pain, vomiting, dyspnea, absent breath sounds, or bowel sounds heard during auscultation of the chest. Information about the mechanism of injury should be obtained from prehospital personnel. In patients involved in motor vehicle crashes, information about the velocity and direction of impact, the severity of vehicular damage, the presence of passenger-compartment intrusion, and the presence or absence of deformity of the steering wheel will be helpful to indicate the severity of the crash. Injuries are graded according to the American Association for the Surgery of Trauma-Organ Injury Scale for Diaphragmatic Injuries (Table 28-3).
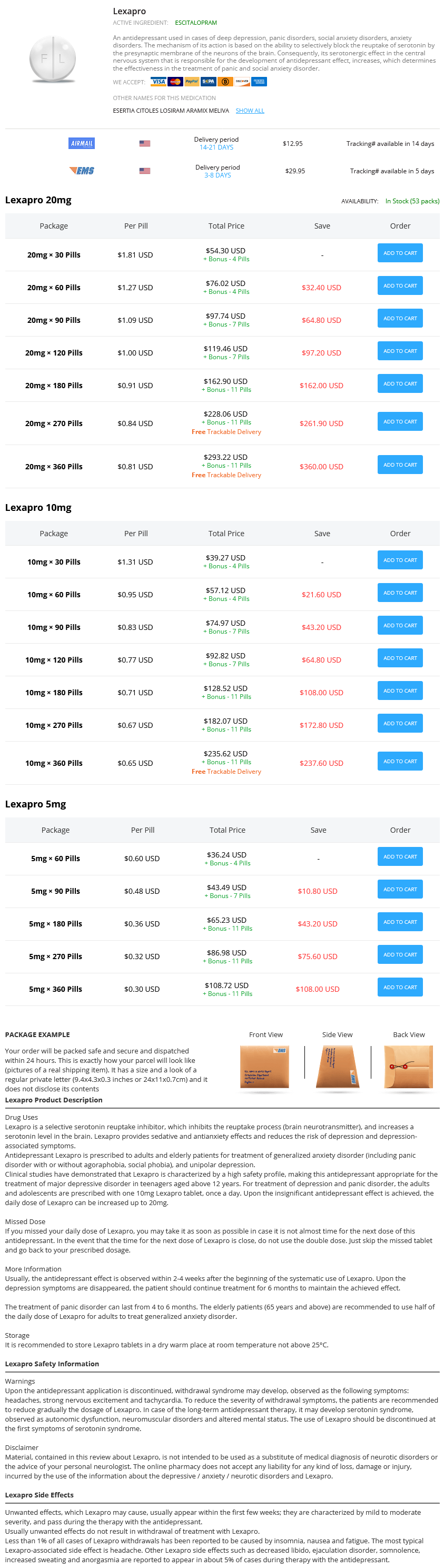
Lexapro Dosage and Price
Lexapro 20mg
- 30 pills - $54.30
- 60 pills - $76.02
- 90 pills - $97.74
- 120 pills - $119.46
- 180 pills - $162.90
- 270 pills - $228.06
- 360 pills - $293.22
Lexapro 10mg
- 30 pills - $39.27
- 60 pills - $57.12
- 90 pills - $74.97
- 120 pills - $92.82
- 180 pills - $128.52
- 270 pills - $182.07
- 360 pills - $235.62
Lexapro 5mg
- 60 pills - $36.24
- 90 pills - $43.49
- 180 pills - $65.23
- 270 pills - $86.98
- 360 pills - $108.72
Visser H anxiety 5 htp buy lexapro online now, et al: Sarcoid arthritis: clinical characteristics, diagnostic aspects, and risk factors. Glennas A, et al: Acute sarcoid arthritis: occurrence, seasonal onset, clinical features and outcome. Korsten P, et al: Druginduced granulomatous interstitial nephritis in a patient with ankylosing spondylitis during therapy with adalim umab. Powell J, et al: Acute systemic sarcoidosis complicating ustekinumab therapy for chronic plaque psoriasis. Gonnelli S, et al: Prevention of corticosteroidinduced osteoporosis with alendronate in sarcoid patients. SaidenbergKermanach N, et al: Bone fragility in sarcoidosis and relationships with calcium metabolism disorders: a cross sectional study on 142 patients. Mirsaeidi M, et al: Racial difference in sarcoidosis mortality in the United States. American Thoracic Society/European Respiratory Society/ World Association of Sarcoidosis and other Granulomatous Disor ders. Biller H, et al: Genotypecorrected reference values for serum angiotensinconverting enzyme. Ohira H, et al: Myocardial imaging with 18Ffluoro2deoxyglucose positron emission tomography and magnetic resonance imaging in sarcoidosis. Gupta D, et al: Endobronchial ultrasoundguided transbronchial needle aspiration vs conventional transbronchial needle aspiration in the diagnosis of sarcoidosis. Atypical osteoarthritis or chondrocalcinosis should trigger a search for an underlying metabolic disorder. Along with anemia, chronic iron deficiency results in a variety of other clinical manifestations such as changes to the nails, tongue, esophagus, and muscles. Of a typical daily Western diet of 10 to 20 mg of iron, 1 to 2 mg is absorbed by duodenal enterocytes each day. The addition of ascorbic acid to the meal increases absorption of nonheme iron, whereas tannins, bran, and phytates inhibit iron absorption. It is then either stored intracellularly and eventually excreted through the feces or absorbed via ferroportin transfer out of the enterocyte, aided by ferroxidase activity of the ceruloplasmin homologue, hephaestin. Communication between sites of iron uptake, utilization, and storage is tightly controlled. Ferroportin facilitates release of intra-cellular iron and is a major player in iron homeostasis, modulated by hepcidin, which plays a central role in the process. Hemochromatosis was first recognized in the 1880s in a series of case reports that described "bronze diabetes" and "pigmented cirrhosis," but von Recklinghausen1 is credited with the first use of the term in 1889. At that time, premorbid recognition of the problem was uncommon, and most cases were diagnosed at autopsy. Autosomal recessive Autosomal dominant Similar to type 1 Hepatic type Macrophage type on hepatocytes. In contrast, inappropriately low hepcidin expression permits increased absorption of iron from the duodenum, high transferrin saturation, and iron overload in sites of tissue storage. Homozygosity for this mutation is a risk factor for organ damage as a result of iron overload, although phenotypic expression varies widely. Clinical manifestations of the latter mutations are less significant, although compound heterozygosity may be associated with evidence of iron overload, particularly if comorbid conditions such as excess alcohol intake or steatosis are present. In the first type, loss of surface localization of ferroportin results in a decreased ability of cells to export iron, causing iron to build up predominantly in macrophages. In the second type, hepcidininduced ferroportin dysfunction leads to iron accumulation in parenchymal cells of the liver and other tissues. In people of African descent, a common polymorphism in the ferroportin 1 gene is associated with mild anemia and a tendency to iron loading. Patients with hereditary hyperferritinemia-cataract syndrome have elevated ferritin levels and bilateral congenital cataracts. Values of serum ferritin exceeding 1000 µg/L are associated with significantly increased risks of liver fibrosis and cirrhosis. Not infrequently, abnormalities of liver enzymes, checked as part of a routine health check, identify the problem. In the liver, increasing iron deposition results in eventual fibrosis and cirrhosis. However, elevated ferritin levels, particularly in the setting of nonalcoholic fatty liver disease, may be associated with vascular damage via hepcidin upregulation. It is a late finding, and the development of "bronze diabetes" represents the end stage of years of iron accumulation in the tissues. High serum iron concentrations may increase bacterial virulence, and excess iron in macrophages is thought to reduce phagocytosis. In addition, Yersinia enterocolitica, Listeria monocytogenes, Salmonella enteritidis serotype typhimurium, Klebsiella pneumoniae, Escherichia coli, Rhizopus arrhizus, and Mucor species all have been reported to cause severe illness in patients with iron overload. Arthritis may be present in the proximal interphalangeal joints, wrists, shoulders, hips, knees, and ankles. Rheumatoid factor is typically negative, however, and in established cases, radiographs show distinctive findings, such as joint space narrowing of the second and third metacarpophalangeal joints, hook-like osteophytes on the radial aspect of the metacarpal heads, and chondrocalcinosis, particularly of the triangular fibrocartilage adjacent to the ulnar styloid. Toxic effects from local iron deposition, acceleration of cartilage defects, and immunologic mechanisms have been implicated. A full history of medication use, including over-the-counter iron tablets, and a review of any blood transfusions should be elicited. Ineffective erythropoiesis in conditions such as the thalassemias or sideroblastic anemia also results in the buildup of iron stores.
© 2025 Adrive Pharma, All Rights Reserved..