General Information about Kamagra
Kamagra is on the market in various types, together with tablets, oral jelly, and chewable tablets. It is taken by mouth and works by inhibiting the enzyme PDE5, which causes the comfort of easy muscular tissues and increases blood circulate to the penis. This results in a agency and long-lasting erection, permitting males with ED to have interaction in sexual exercise with none difficulty.
In conclusion, Kamagra is a highly useful medicine for the therapy of ED and PAH. It has revolutionized the treatment of ED and has helped many males regain their sexual confidence and improve their high quality of life. It is necessary to note that it should solely be taken underneath the steering of a healthcare professional and should not be used with no prescription. If you're experiencing symptoms of ED or PAH, talk to your doctor about whether Kamagra may be an acceptable therapy possibility for you.
Erectile dysfunction is a standard situation that impacts hundreds of thousands of men worldwide. It is characterized by the shortcoming to attain or maintain an erection firm sufficient for sexual intercourse. This can have a significant impact on a man's vanity, relationships, and overall high quality of life. While ED may be brought on by numerous elements such as stress, nervousness, and sure medical situations, it is primarily as a end result of restriction of blood circulate to the penis.
Aside from ED, Kamagra is also used within the treatment of PAH, a condition in which the blood vessels within the lungs become slender, stiff, or blocked. This puts a strain on the guts and can result in shortness of breath, fatigue, and chest pain. By stress-free the blood vessels within the lungs, Kamagra helps to enhance blood flow and relieve signs of PAH.
Clinical research have shown that Kamagra is very effective in treating ED in men of all ages. In truth, it has an 80% success rate in bettering erectile operate. It is also a secure and well-tolerated medicine, with the most common side effects being headache, nausea, and dizziness. However, it is essential to seek the guidance of a healthcare professional before taking Kamagra, as it could work together with certain drugs or have opposed results in individuals with sure medical conditions.
Kamagra, also known as sildenafil, is a medicine commonly used for the therapy of erectile dysfunction (ED) in men. It can additionally be prescribed for pulmonary arterial hypertension (PAH), a situation that impacts the guts and lungs. Kamagra belongs to a class of medicine generally identified as phosphodiesterase sort 5 (PDE5) inhibitors, which work by relaxing the blood vessels and rising blood circulate to the penis or lungs.
While Kamagra is primarily used for the remedy of ED and PAH, it has additionally been found to have other potential advantages. Some research have shown that it may improve exercise efficiency and improve oxygen levels in the blood. It is also being investigated for its potential use in treating altitude sickness and Raynaud's phenomenon, a condition that causes the blood vessels in the fingers and toes to narrow.
Most studies on the efficacy of manipulation utilize about two treatments per week for two to three weeks impotent rage definition 50 mg kamagra sale. The goals of massage therapy include sedation, adhesion reduction, fluid mobilization, muscular relaxation, and vascular changes. Combining massage therapy with education and exercises may be better than using massage therapy alone. This advantage has to be tempered by the fact that these are generally passive treatments which can, if overused, contribute to deconditioning. Physical modalities often have a relaxing effect in addition to temporarily controlling pain which gives them the potential for abuse. Ideally, they should be used as adjuncts to the rehabilitative process and their efficacy assessed in terms of their contribution to the overall goals of maximizing function and quality of life. Spinal manipulation In the United States, manual medicine encompasses a variety of techniques. This, combined with use while lying down, have resulted in burns after patients fell asleep. Vasoconstriction, decreased nerve conduction, decreased tendon extensibility, and increased joint stiffness add to an analgesic effect and general relaxation. Intermittent ice application (on for ten minutes, off for five minutes, on for ten minutes) may be superior to one 20-minute treatment. Candidates for traction include those with discogenic radiculopathy and an x-ray that reveals no evidence of serious spine disease. These successful programs share several key components including intensive physical training. The training for these workers, who are typically either off work or in modified duties, is oriented to specific work tasks. Modifying maladaptive beliefs and attitudes, and addressing distress, changes behavior and thus disability. They easily hang from a belt or fit in a pocket, with electrodes attached to the back. In addition, these programs even outside the Chapter 37 Chronic back pain] 511 work-hardening arena are perhaps one of the most useful tools for the spine clinician. First, the back pain and radicular leg pain component are approached as two different problems since they can act and respond to treatments in very different ways. For instance, the back pain component does not usually respond to the treatments that are helpful for the radicular component. Treatments, such as surgical discectomy, epidural steroid injections, or neuropathic drugs, can eliminate radicular leg pain, but have not shown efficacy for treating axial pain. Occasionally, the radicular pain comes from a synovial cyst, but serious underlying spine disease as a source of radiculopathy is extremely rare32 and only investigated if the usual low back screening red flags are positive. The natural history of discogenic radiculopathy is one of complete elimination of leg symptoms over time. The least invasive treatment options involve physical therapy combined with anlagesic oral medications. The therapy can generally consist of paincontrol treatments via modalities like heat, ice, or electrical stimulation, foraminal opening maneuvers, a trial of McKenzie techniques, education on back care, sleeping positions, body mechanics, stretches, and possibly a trial of traction. Analgesics are similar to those discussed above under Medication, with the addition of medications specific for treating neuropathic pain, such as gabapentin, pregabalin, duloxetine, tramadol, or tricyclic antidepressants. For patients who have not responded adequately to these types of treatments over time, fluoroscopically guided and contrast-controlled injections into the epidural space may add additional pain control. Empirically, patients are limited to three injections a year to avoid steroid side effects. Injections are approached one at a time and efficacy is evaluated ten days to two weeks later before any repeat injections are considered. For patients with predominantly leg pain and continued disability despite treatments as described, a surgical consultation could be offered. Patients with classical spinal stenosis may well have significant back pain, but they usually present because of bilateral leg pain that limits their standing and walking (pseudoclaudication). Various spine injections should be considered a stepping stone to one of these main treatments, not used in isolation. Many patients find such dramatic relief with a facet joint injection or sacroiliac joint block that they abandon all other treatments until pain returns weeks or months later. This is a debatable issue as efficacy data in general are conflicting and of poor quality. Many suggest that variability of techniques used and in particular the lack of image-guidance for epidural injections, is a big factor behind these study results. Looking at the 15 randomized trials on the efficacy of epidural corticosteroid injections for discogenic radiculopathy, systematic reviews are conflicting. They should only be performed with the intent to move along the rehabilitation process, after proper screening for contraindications, and executed in experienced hands. This is carried out in addition to the usual back pain treatments described above under Setting up a sound treatment program. Many patients find that using a walker to allow some forward flexion while walking, increases walking tolerance significantly. Oral analgesics or epidural corticosteroid injections may be of benefit especially if there is a significant discogenic component to the stenotic area of the spinal canal. Surgery is considered an elective procedure which should ultimately be offered based on disability and lack of medical contraindications. This is a controversial area of medicine highlighted by recent published expert opinion statements critical of spinal fusion surgery146[V] and in response, supportive of surgery. History, examination, and imaging or provocative discography studies do a poor job at differentiating patients with truly discogenic pain from others.
Spinal cord stimulation for refractory angina pectoris: a retrospective analysis of efficacy and cost-benefit erectile dysfunction ayurvedic drugs buy kamagra with paypal. Comparison of transmyocardial revascularization with medical therapy in patients with refractory angina. Transmyocardial revascularization with a carbon dioxide laser in patients with end-stage coronary artery disease. The effects of transcutaneous electrical nerve stimulation in patients with severe angina pectoris. A prospective, multicenter randomized trial of percutaneous transmyocardial laser revascularization in patients with non-recanalizable chronic total occlusions. Usefulness and safety of percutaneous myocardial laser revascularization for refractory angina pectoris. Treatment of medically and surgically refractory angina pectoris with high thoracic epidural analgesia: initial clinical experience. Long term benefits of stellate ganglion block in severe chronic refractory angina. Endoscopic thoracic sympathectomy its effect in the treatment of refractory angina pectoris. A brief cognitivebehavioural intervention reduces hospital admission in refractory angina pectoris. The effects of sympathectomy on the electrocardiogram and effort tolerance in angina pectoris. Effects of spinal cord stimulation on regional myocardial perfusion assessed by positron emission tomography. Long-term outcome of spinal cord electrical stimulation in patients with refractory chest pain. Temporary cessation of spinal cord stimulation in angina pectoris effects on symptoms and evaluation of long-term effect determinants. Refractory angina pectoris in end-stage coronary artery disease: Evolving therapeutic concepts. Psychosocial factors associated with noncardiac chest pain and cardiac syndrome X. Spinal cord stimulation in patients with refractory angina pain and normal coronary arteries. Antianginal and antiischaemic effects of nisoldipine and ramipril in patients with syndrome X. Acute and mid-term combined hormone replacement therapy improves endothelial function in post-menopausal women with angina and angiographycally normal arteries. Electrical neuromodulation improves myocardial perfusion and ameliorates refractory angina pectoris in patients with syndrome X. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Intrapericardial treatment of autoreactive pericardial effusion with triamcinolone. Esophageal function in patients with angina-type chest pain and normal coronary angiograms. Effects of omeprazole versus placebo in treatment of noncardiac chest pain and gastroesophageal reflux. Diagnostic value of esophageal studies in patients with angina-like chest pain and normal coronary angiograms. Oral nifedipine in the treatment of noncardiac chest pain in patients with the nutcracker esophagus. Low-dose trazodone for symptomatic patients with esophageal contraction abnormalities. Treatment of chest pain in patients with noncardiac, nonreflux, nonachalasia spastic esophageal motor disorders using botulinum toxin injection into the gastroesophageal junction. Stress induces alteration of esophageal pressures in healthy volunteers and non-cardiac chest pain patients. Musculoskeletal chest wall syndromes in patients with noncardiac chest pain: a study of 100 patients. Costal chondritis in heroin addicts: a comparative study with post-surgical chondritis. Can early diagnosis and management of costochondritis reduce acute chest pain admissions Research designs in interventional pain management: Is randomisation superior, desirable or essential Prevalence of facet joint pain in chronic spinal pain of cervical, thoracic and lumbar regions. Thoracic zygoapophyseal joint pain: a review and description of an intraarticular block technique. Visceral pain is poorly localized and evokes strong autonomic and emotional responses. There is poor correlation between visceral pathology and the principles of the management of visceral pain are similar to those of other painful conditions. These pains fall within the practice of virtually every medical specialty and are some of the most common presenting symptoms for the primary care physician. Pain experienced in the abdomen, groin, and/ or perineum may arise from pathology of the nervous system innervating those structures or may originate in the viscera, vascular structures or musculoskeletalarticular stuctures in the region.
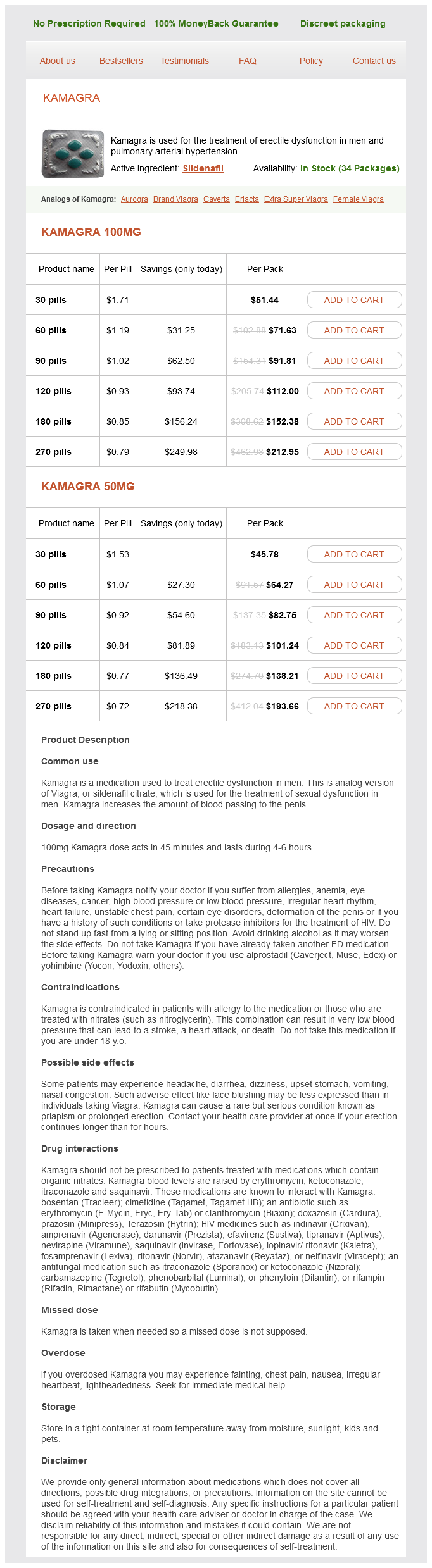
Kamagra Dosage and Price
Kamagra 100mg
- 30 pills - $51.44
- 60 pills - $71.63
- 90 pills - $91.81
- 120 pills - $112.00
- 180 pills - $152.38
- 270 pills - $212.95
Kamagra 50mg
- 30 pills - $45.78
- 60 pills - $64.27
- 90 pills - $82.75
- 120 pills - $101.24
- 180 pills - $138.21
- 270 pills - $193.66
Pain treatment related to inflammatory bowel disease forms a limited-choice corollary to chronic pancreatitis (Box 40 erectile dysfunction after radiation treatment for prostate cancer buy cheap kamagra line. Since reports of pain may be associated with life-threatening complications, these patients may have frequent hospitalizations. The use of opioids and other motility-altering drugs carries the perception of an increased risk of toxic dilation with an associated increase in morbidity and mortality. Similar to other diseases with unknown etiologies, genetic influences, immunologic abnormalities, and infectious agents have all been implicated and used as rationales for treatment. Primary treatment for exacerbations is typically bowel rest, anti-inflammatories. Multiple therapies such as oral sulfasalazine, oral mesalazine, oral olsalazine, oral metronidazole, systemic corticosteroids, and mesalamine enemas/suppositories have been utilized not only as reactive treatments for exacerbations but as prophylactic measures. Immunosuppressants such as azothioprine, methotrexate, and cyclosporine have been used for a presumed immunologic etiology. Recent use of drugs known to affect inflammatory responses in rheumatological disorders has been encouraging101 with successful clinical trials reported for infliximab102 but not for etanerecept. Psychological treatments are justified by the presence of a life-long, recurrent disease process. A similar phenomenon has been noted in the gastrointestinal system whereby severe abdominal pain may be precipitated by the ingestion of a meal. Poor peripheral pulses, abdominal bruits, and arteriographic evidence of stenosis or occlusion in the three main mesenteric arteries are all consistent with the diagnosis of abdominal angina. Similar to cardiac disease, abdominal angina may precede infarction which has devastating life-threatening consequences. Arterial thrombosis, embolic events, venous occlusion, and low flow states due to poor cardiac output may all lead to the same disastrous results. Ischemic colitis represents approximately half of the cases of morbidity due to mesenteric vascular disease. Although usually diagnosed by colonoscopy, 20 percent of patients with ischemic colitis develop evidence of peritonitis requiring surgical diagnosis and treatment. Initial presentation may be with persistent diarrhea, rectal bleeding, or weight loss. Diagnostic work-up for mesenteric ischemia has angiography as the gold standard, but the less invasive magnetic resonance angiography and/or tonometry have diagnostic value. Pharmacologically, there can be short-term value of vasodilators such as papverine and, like most chronic processes with some low grade inflammatory component, there appears to be a role for the use of antioxidants and agents acting via cytokine mechanisms, but at present these treatments are experimental. Bleeding diverticuli are the most common sources of lower gastrointestinal tract bleeding113 and segmental colonic resection has the highest success rate at stopping bleeding. Reports of pain do not always correlate with observable pathology and symptoms can be nonspecific. Linked to alterations in the innate immune system involving the protein pyrin, the pathogenesis of this and other periodic fever syndromes is still being defined. Abdominal pain of varying intensity occurs in 95 percent of the episodes with chest pain and arthralgias in 75 percent of episodes. The frequency of the episodes may vary from twice per week to once per year, but most commonly occur at two- to fourweek intervals with acute episodes typically lasting between one and three days. Amyloidosis with associated kidney failure and athralgia are the most severe associated sequelae. Typical treatment is episodic with the use of systemic analgesics although case reports support use of modalities such as intermittent spinal cord stimulation. Diverticular disease Diverticuli can occur throughout the gastrointestinal tract but prove to be most common in the colon where they exist as small sac-like herniations of mucosa through the muscular wall, typically at the site of penetrating blood vessels. Colonic diverticuli are generally pain free but with the development of inflammation and/ or obstruction of their mouth, severe abdominal pain and infection may result. Peridiverticular abscesses, obstruction, colonic distension, bleeding, and altered bowel habit (diarrhea, constipation) are not uncommon. Painful diverticulosis classically presents as recurrent left lower quadrant colicky pain without evidence of inflammation. Like chronic pancreatitis, diverticular disease can produce Porphyria Several related genetic disorders, all characterized by the increased formation of porphyrins or their precursors, are Chapter 40 Chronic abdominal, groin, and perineal pain of visceral origin] 563 termed porphyria122, 123 (Box 40. Transmitted as an autosomal dominant disorder with incomplete penetrance, family history may or may not be helpful in the diagnosis. Neurological dysfunction may occur principally due to demyelination effects with emotional disturbance a nonspecific symptom. Most opioids are alleged to be nontriggering, a notable exception is the mixed agonistantagonist pentazocine. Chlorpromazine, promethazine, and droperidol have all been reported to be safe as antiemetics. Hallmark features consist of persistent complaints of urinary urgency, dysuria, poor urinary flow, and perineal discomfort without evidence of bacteria or white blood cells in prostatic fluids. It serves as a male-specific corollary to interstitial cystitis in that it has similar symptomatology, is a diagnosis of exclusion, and has a presumed site of pain generation. Infectious, inflammatory, neurological, and referred gastroenterological etiologies of the pain need to be ruled out. Cystoscopic findings of interstitial cystitis have been found in males with the diagnosis of prostatodynia. As with interstitial cystitis, treatments may be empiric trials of medications employed in the treatment of any other chronic pain. Antibiotics are commonly employed despite the absence of evidence for a microbiological etiology.
© 2025 Adrive Pharma, All Rights Reserved..