General Information about Kamagra Polo
Kamagra Polo has a quick onset of motion, with results kicking in within 15-30 minutes after consumption. This is far quicker than other ED medications, which can take up to an hour to begin working. This attribute makes it the proper selection for spontaneous sexual exercise, providing men with the boldness and reassurance they want to carry out sexually.
Kamagra Polo can be a cost-effective possibility for treating ED. It is significantly cheaper than the branded Viagra, without compromising on its efficacy and security. This makes it a more accessible possibility for males who cannot afford or do not have insurance coverage protection for costly ED medicines.
In conclusion, Kamagra Polo is a revolutionary answer for erectile dysfunction. It is a protected, effective, and convenient remedy possibility that gives men with fast and long-lasting reduction from ED. With its unique type, quick onset of motion, and longer period of impact, Kamagra Polo has gained reputation worldwide as a dependable alternative for men coping with ED. If you're struggling with this condition, don't hesitate to talk to your doctor about Kamagra Polo and see how it can improve your sexual health and general well-being.
One of the primary advantages of Kamagra Polo is its convenient and discreet form. The pill is formed like a polo mint, and it can be simply chewed and swallowed, with out the necessity for water. This makes it a super possibility for males who have difficulty swallowing drugs. Additionally, it is out there in numerous fruity flavors such as pineapple, orange, strawberry, and mint, making it more interesting for individuals who dislike the bitter taste of typical ED medications.
Kamagra Polo is an oral treatment that is particularly designed to treat ED and its signs. It is a chewable version of the well-known medicine, Viagra, and is manufactured by Ajanta Pharma, a famend pharmaceutical company. Kamagra Polo incorporates the lively ingredient Sildenafil Citrate, which belongs to a bunch of medicines called phosphodiesterase kind 5 (PDE5) inhibitors. It works by rising blood move to the penis, allowing for a stronger and longer-lasting erection.
Like any medication, Kamagra Polo might trigger some side effects, that are often mild and temporary. The most typical unwanted effects embrace headaches, dizziness, facial flushing, and indigestion. These side effects sometimes subside because the medication wears off, and they are often easily managed by staying hydrated and avoiding alcohol consumption. It is important to seek the assistance of a doctor before taking Kamagra Polo, particularly if an individual has any underlying medical circumstances or is taking another medicines.
Kamagra Polo: A Revolutionary Solution for Erectile Dysfunction
Erectile dysfunction (ED) is a common drawback affecting men of all ages. It refers to the incapability to realize or preserve an erection that is firm sufficient for sexual intercourse. This situation may cause vital misery and have a unfavorable impact on a man's shallowness and their intimate relationships. Fortunately, there are various therapy options obtainable, and one such resolution is Kamagra Polo.
Moreover, Kamagra Polo has a longer length of motion, with results lasting as much as 6 hours. This means that men can get pleasure from multiple sexual encounters inside a brief while, with out having to fret about dropping their erection. However, it's essential to notice that Kamagra Polo won't cause an erection except there could be sexual stimulation present.
With this clinical presentation low testosterone erectile dysfunction treatment order kamagra polo 100 mg mastercard, the differential diagnosis includes neuroretinitis (cat-scratch disease, toxoplasmosis), diabetic papillopathy, and optic neuritis of infectious (sarcoidosis, syphilis, Lyme disease) or inflammatory etiology. Often, headache is present in patients with malignant hypertension; nevertheless, papilledema secondary to intracranial disease also presents with headache and must be ruled out. Because these features represent permanent changes in the vessel walls, they persist long after blood pressure has normalized. In contrast, the acute manifestations indicate poor blood pressure control at the time of the ocular examination. Retinal hemorrhages and cotton-wool spots would be expected when the autoregulatory mechanisms of the retinal arterioles are overwhelmed. In normal individuals, this occurs when the mean arterial blood pressure rises suddenly above 115 mm Hg. Management consists of controlling the blood pressure; appropriate systemic therapy leads to resolution of the acute, potentially sight-threatening manifestations. Some degree of permanent visual loss may be encountered if there is significant macular or optic nerve involvement. When there are signs of severe hypertensive retinopathy, choroidopathy, or any optic nerve head swelling, the blood pressure must be checked in the office immediately. Very high systemic blood pressure is a medical emergency and necessitates prompt referral to a comprehensive health care facility. Gradually, the intima is replaced by hyaline and the muscular wall becomes fibrotic. In addition, focal areas of capillary nonperfusion to the nerve fiber layer result in ischemic zones, which appear as cotton-wool spots. Cotton-wool spots appear white because of axoplasmic stasis in the area of retinal ischemia. Blood pressure should be checked immediately in the office and the patient referred promptly if uncontrolled hypertension is confirmed. He classified patients having the disease into three groups with varying degrees of vascular abnormality, but all with massive subretinal exudates. Group 3 patients had arteriovenous malformation and exudation, which von Hippel later characterized as a distinct entity, angiomatosis retinae, leading Coats to remove it from his classification. He was also the first to use the term retinal telangiectasis, which many authors feel better describes the disease and its wide spectrum of presentations and varying degrees of severity. Because of the common presentation of leukocoria and strabismus in other childhood diseases, other diagnoses must be investigated (Table 13. The term retinal telangiectasis is appropriate, as this is a disease principally of the retinal capillaries. However, larger vessels, including large arteries and veins, can be affected with sheathing, aneurysmal dilations, and exudation. Interestingly, retinal neovascularization is rare despite the presence of capillary nonperfusion and adjacent, relatively normal blood vessels. Vitreous hemorrhage and neovascularization are seen only when larger zones of capillary nonperfusion or retinal detachment are present. Often, the ophthalmoscopic and angiographic picture in the adult form of disease is difficult to differentiate from that of other perifoveal microvascular abnormalities (Table 13. Exudative retinal detachment typical of the childhood form is rarely seen in adults. Initially, severe retinal vascular leakage causes subretinal deposition of protein and lipid-rich exudate. In fact, disciform scars are most common in children and infants with broader zones of peripheral involvement. Cataract, iridocyclitis, neovascular glaucoma, and eventually phthisis bulbi can occur. Rarely, organization of subretinal fluid in long-standing detachments can lead to a clinical picture simulating that of other diseases. Coalescence of intraretinal cystic spaces in unresolved detachments have reportedly led to hemorrhagic retinal macrocysts. Delayed time shots represent increased time for gastrointestinal absorption of fluorescein. Multiple reports of an association with muscular dystrophy, and more recently with facioscapulohumeral dystrophy, exist. Large areas of capillary nonperfusion are typically associated with neighboring abnormal large vessels with aneurysmal dilations. Large zones of exudative retinal detachment distal to the telangiectasias do not stain. However, fluorescein dye does fill intraretinal cystic spaces, often showing a pattern characteristic of cystoid macular edema. Most recently, ultrawide-field 189 Diseases of the Vitreous, Retina, and Choroid color fundus and fluorescein imaging has contributed to a greater understanding of this spectrum of peripheral retinal vascular disease, particularly in the realm of pediatric retina. Single-shot images of the posterior pole and retinal periphery are obtained quickly without the need for examination under anesthesia. Endophytic retinoblastomas may have a feeder vessel leading to the subretinal mass. Unsuspected areas of vascular leakage can be readily identified, and treatment in the form of photocoagulation or cryotherapy then directed to those areas (see Management and Course). The differential diagnosis includes all perifoveal retinal microvascular abnormalities that can present with or without leakage (see text box). Cavernous hemangioma is a relatively discrete retinal vascular anomaly that can be likened to a cluster of grapes. Acquired arterial macroaneurysms have a zone of leakage typically surrounding a single lesion by angiography.
Traction is released by removing the organized vitreous ridge-to-ridge erectile dysfunction with normal testosterone levels order kamagra polo online pills, ridge-toperiphery, ridge-to-lens, and ridge-to-disc. If there is persistent plus disease, with engorgement of the iris vasculature and tortuosity and dilation of the retinal vessels, the risk for intraoperative hemorrhage can be higher. The detachment occurs because of failure of the ablation to arrest the progression of tractional retinal detachment. Nonetheless, ablative therapy usually induces regression of severe plus disease, making subsequent vitreous surgery safer. Patients are treated initially with peripheral avascular retinal ablation, and this area of treated retina usually does not detach; the configuration of retinal detachments in treated patients is typically such that a peripheral trough forms, with the more anterior avascular retina remaining attached. In approximately 3 weeks, plus disease has generally regressed to the point where vitreous surgery can be performed. The tissues can be segmented and left in place if the vitreoretinal tractional forces have been relieved. Retinal breaks occur most often anteriorly in the region of the pars plana during dissection of very adherent epiretinal membranes. When a retinal break occurs, flattening of the retina to permit adequate cryotherapy or laser around the break and on the retina in the area of the scleral buckle is difficult. In none of the cases reported by Zilis et al116 in which a retinal break was noted during surgery did reattachment occur. When a retinal break is not seen but schlieren (small masses or streaks occurring when two clear fluids of different optical densities mix) is observed, a retinal break should be assumed to be present-although pockets of denser fluid can reside within areas enclosed by membranes or folds and may present with schlieren-like appearances when liberated. For stage 4B, posterior pole distortion should be minimized as much as possible, but macular dragging will be common, total retinal reattachment may not be possible in most cases, and the lens may have to be sacrificed in some cases. Staged approaches can be taken by performing a lensectomy and external drainage on the first surgery and returning several weeks later to work on membrane dissection. Determining the configuration of the retinal detachment is the first essential step in surgical planning. Disadvantages of open-sky vitrectomy include lack of control of intraocular pressure and difficulty in posterior manipulation. Currently, open-sky vitrectomy may be appropriate for eyes with cloudy corneas that prevent closed vitrectomy or for eyes with very narrow-funnel stage 5 retinal detachments. The basic steps include trephining the cornea, extracting the lens with a cryoprobe, and then dissecting the epiretinal fibrous proliferation stepwise in an anterior-to-posterior direction. Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. The incidence and course of retinopathy of prematurity: findings from the early treatment for retinopathy of prematurity study. Extreme prematurity and fibroblastic overgrowth of persistent vascular sheath behind each crystalline lens. Further studies on fibroplastic overgrowth of the persistent tunica vasculosa lentis. Intensive oxygen therapy as a possible cause of retrolental fibroplasia; a clinical approach. Characteristics of infants with severe retinopathy of prematurity in countries with low, moderate, and high levels of development: implications for screening programs. Regulation of vascular endothelial growth factor by oxygen in a model of retinopathy of prematurity. Vascular abnormalities in aggressive posterior retinopathy of prematurity detected by fluorescein angiography. Fluorescein angiography of recurrent retinopathy of prematurity after initial intravitreous bevacizumab treatment. Atlas of fluorescein angiographic findings in eyes undergoing laser for retinopathy of prematurity. Optical coherence tomography in the management of acute retinopathy of prematurity. Optical coherence tomography findings in stage 4A retinopathy of prematurity: a theory for visual variability. Insights into advanced retinopathy of prematurity using handheld spectral domain optical coherence tomography imaging. Retinoschisis detected with handheld spectral-domain optical coherence tomography in neonates with advanced retinopathy of prematurity. Understanding clinically undetected macular changes in early retinopathy of prematurity on spectral domain optical coherence tomography. Spectral-domain optical coherence tomographic assessment of severity of cystoid macular edema in retinopathy of prematurity. Subclinical macular findings in infants screened for retinopathy of prematurity with spectral-domain optical coherence tomography. Evaluation of optic nerve development in preterm and term infants using handheld spectral-domain optical coherence tomography. Poorer neurodevelopmental outcomes associated with cystoid macular edema identified in preterm infants in the intensive care nursery. Three-dimensional assessment of vascular and perivascular characteristics in subjects with retinopathy of prematurity. Telemedical evaluation and management of retinopathy of prematurity using a fiberoptic digital fundus camera. Telemedicine approach to screening for severe retinopathy of prematurity: a pilot study.
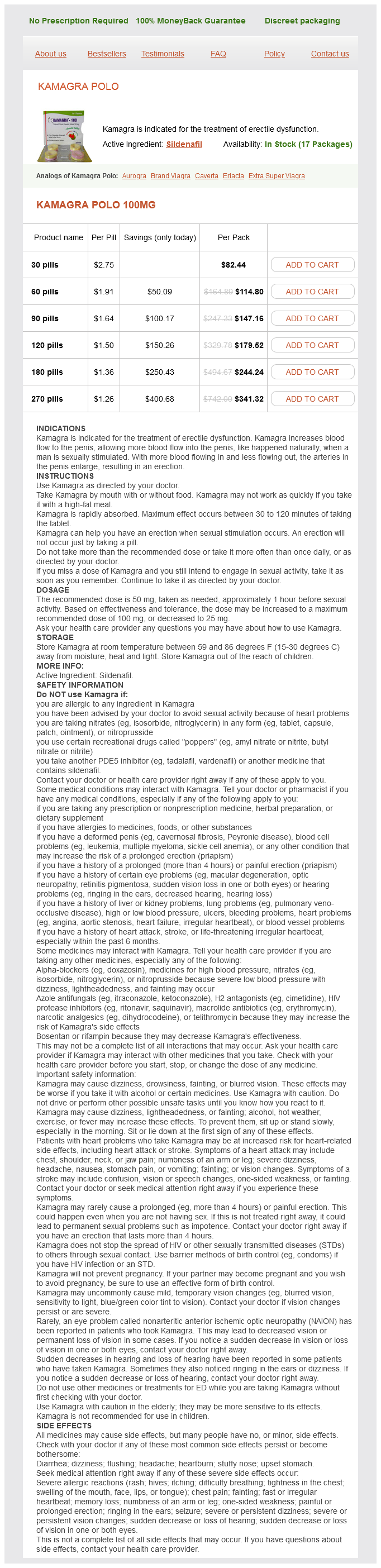
Kamagra Polo Dosage and Price
Kamagra Polo 100mg
- 30 pills - $82.44
- 60 pills - $114.80
- 90 pills - $147.16
- 120 pills - $179.52
- 180 pills - $244.24
- 270 pills - $341.32
Intestinal calcium-binding protein and calcium absorption in cortisol-treated chicks: effects of vitamin D3 and 1 impotence 35 years old buy 100 mg kamagra polo,25-dihydroxyvitamin D3. Regulation of vitamin D-1alpha-hydroxylase and -24-hydroxylase expression by dexamethasone in mouse kidney. Influence of thyroid function on the serum concentration of 1,25-dihydroxyvitamin D3. Human fibroblast growth factor-23 mutants suppress Na+-dependent phosphate co-transport activity and 1alpha,25-dihydroxyvitamin D3 production. Elevated 1,25-dihydroxyvitamin D plasma levels in normal human pregnancy and lactation. Dynamic changes in circulating 1,25-dihydroxyvitamin D during reproduction in rats. The signal sequence, along with the short prosequence, functions to direct the protein into the secretory pathway. Like other signal sequences, the presequence binds to a signal recognition particle during protein synthesis. The signal recognition particle then delivers the nascent peptide chain to the rough endoplasmic reticulum, where it is threaded through a protein-lined aqueous pore. During this transit, the signal sequence is cleaved off by a signal peptidase, and the presequence is rapidly degraded. The amino acid sequence has been determined in several species, and there exists a high degree of identity among species, particularly in the amino-terminal region of the molecule. This protein, secretory protein I, is identical to chromogranin A isolated from the adrenal medulla, and it is present in other endocrine cells and neoplasms as well. It is therefore likely that they arose from a common precursor by chromosomal duplication [19]. The physiological relevance of these findings was established by in vivo studies in rats [2]. This effect was shown to be transcriptional both in in vivo studies in rats [2] and in in vitro studies with primary cultures of bovine parathyroid cells [44]. Studies of gene knockout mice have shown that the hoxa3, pax 1, pax 9, and Eya1 transcription factors are needed to form parathyroid glands as well as many other pharyngeal pouch derivatives, such as the thymus [25]. Glial cells missing 2 (Gcm-2), a mouse homologue of Drosophila Gcm, is a transcription factor whose expression is restricted to the parathyroid glands [32]. The parathyroid gland of tetrapods and the gills of fish both express Gcm-2 and require this gene for their formation [36]. Hypocalcemic rats had increased levels of calreticulin protein, as measured by Western blots, in their parathyroid nuclear faction [48]. The CaR is expressed in parathyroid chief cells, thyroid C-cells, and cells of the kidney tubule, and is essential for maintenance of calcium homeostasis. Drueke has analyzed the clinical trials that have been performed and concluded that all clinical studies were retrospective in nature and suffered from the limitations of retrospective data analysis [63]. The development of calcimimetic drugs that act Calcium Receptor and Vitamin D Receptor Interactions in the Parathyroid Russell et al. Most, but not all, of the phenotype can be reversed by correcting the serum calcium concentration with a high calciumlactose diet [70]. In both the total knockout and the parathyroid-specific knockout mice there was a decrease in parathyroid calcium receptor (CaR) levels. Signal transduction from the CaR involves activation of phospholipase C, D, and A2 enzymes [76]. The response to changes in serum calcium involves the protein phosphatase type 2B, calcineurin [77]. Phosphate Regulates the Parathyroid Independently of Calcium and 1,25-Dihydroxyvitamin D3 the demonstration of a direct effect of high phosphate on the parathyroid in vivo has been difficult. One of the reasons is that the various maneuvers used to increase or decrease serum phosphate invariably leads to a change in the ionized calcium concentration. However, the very low serum phosphates in these in vivo studies may have no direct relevance to possible direct effects of high phosphate in renal failure. It is necessary to separate nonspecific effects of very low phosphate from true physiologic regulation. To establish that the effect of serum phosphate on the parathyroid was indeed a direct effect, in vitro confirmation was needed, which was provided by three groups. This remarkable sensitivity of the parathyroid to increase hormone secretion after small decreases in serum calcium levels is unique to the parathyroid. All other endocrine glands increase hormone secretion after exposure to a high extracellular calcium. These results emphasize that the gland is geared to respond to hypocalcemia and less so to hypercalcemia. In hypocalcemia or uremia, the peptidylprolyl cis/trans isomerase Pin1 is inactive. The requirement for intact tissue suggests either that the sensing mechanism for phosphate is damaged during the preparation of isolated cells or that the intact gland structure is important to the phosphate response. Parathyroid responds to changes in serum phosphate at the level of secretion, gene expression, and cell proliferation, although the mechanism of these effects is unknown. This effect would act as a counterbalance to the stimulatory effect of phosphate on the parathyroid and is discussed separately in this chapter. Fibroblast Growth Factor 23 and the Parathyroid Fibroblast Growth Factor 23 Decreases Parathyroid Hormone Expression Phosphate homeostasis is maintained by a counterbalance between efflux from the kidney and influx from the intestine and bone. Klotho protein is expressed not only in the kidney but also in the parathyroid, pituitary, and sinoatrial node [91].
© 2025 Adrive Pharma, All Rights Reserved..