General Information about Indomethacin
Initially developed in the Nineteen Sixties, indomethacin has since proven to be an efficient medicine for a variety of situations and has been accredited by the U.S. Food and Drug Administration (FDA) for various uses. It is often prescribed for the treatment of circumstances corresponding to gout, complications, rheumatoid arthritis, osteoarthritis, and ankylosing spondylitis.
In conclusion, indomethacin, or Indocin, is a commonly prescribed NSAID that has been confirmed to be an effective treatment possibility for varied forms of ache and inflammation. It should at all times be used as directed by a healthcare provider, and it is crucial to follow the recommended dosage and frequency of use to avoid potential unwanted effects. With its widespread availability and proven effectiveness, indomethacin remains an important medicine within the administration of pain and inflammation.
Indomethacin, additionally known by its brand name Indocin, is a non-steroidal anti-inflammatory drug (NSAID) commonly used to alleviate ache, cut back fever, and reduce irritation. It belongs to a category of medicines known as arylacetic acid derivatives, which work by inhibiting the production of prostaglandins – hormone-like substances responsible for causing ache and irritation in the physique.
Indomethacin works by blocking the enzymes answerable for producing prostaglandins, thus lowering their levels in the body. This, in flip, results in a discount in pain, fever, and irritation, making it an efficient option for managing signs associated with varied conditions.
This medication is primarily used for short-term relief of signs, and it is not beneficial for long-term use due to the threat of potential unwanted side effects. Common unwanted facet effects of indomethacin embody stomach upset, diarrhea, and dizziness. More serious unwanted aspect effects similar to gastrointestinal bleeding and liver or kidney issues have additionally been reported, however these are less common.
Indocin is obtainable in completely different forms, including oral capsules, suppositories, and a liquid solution. Depending on the condition being handled, the dosage and frequency of use may differ. It is usually recommended to take indomethacin with food, as it could cause stomach upset if taken on an empty abdomen.
In addition to its pain-relieving properties, indomethacin has additionally been discovered to have potential anti-cancer results. Studies have proven that it may possibly inhibit the expansion of tumor cells in varied forms of most cancers, together with breast, colon, prostate, and ovarian most cancers. However, extra research is required in this space to discover out its full potential.
Indomethacin should be used with caution in individuals with a history of heart illness, high blood pressure, or kidney problems. It is also not beneficial to be used in pregnant ladies, notably through the third trimester, as it might possibly trigger hurt to the unborn baby. It is at all times important to seek the guidance of a healthcare provider earlier than beginning any new medication, particularly during being pregnant.
In addition arthritis uk knee exercises indomethacin 75 mg amex, oxidant substances and polycyclic aromatic hydrocarbons can potentially play a role. Caffeine, a methylxanthine compound that is chemically similar to theophylline, increases neurohormonal and sympathetic stimulation. The underlying mechanism probably is related to sympathetic activation and reduced coronary microcirculation. Ethanol can lead to electrical atrial remodeling, resulting in slowing of intraatrial conduction and abbreviation of atrial refractoriness. Other potential mechanisms include sympathetic stimulation, modulation of vagal tone, alterations in oxidative stress, electrolyte imbalances (hypokalemia, hypomagnesemia), and alcohol-induced cardiomyopathy. Furthermore, ethanol and its metabolite, acetaldehyde, have direct cardiotoxic effects, including direct effects on atrial excitation-contraction coupling, inhibition of calcium release from the sarcoplasmic reticulum, generation of oxidative stress, accelerated protein catabolism, and derangements in fatty acid metabolism and transport. However, despite its usually transient nature, the arrhythmia is not limited to the early postoperative phase, and can recur between day 6 and day 30 after the operation in about 25% of patients. Loss of effective atrial contraction can potentially reduce cardiac output by 15% to 25%. Such complaints should not be dismissed as "unrelated," and those patients should not be labeled "asymptomatic. Pacemaker interrogation strips from three different patients with dual-chamber pacemakers. Rapid and irregular ventricular response is observed on the ventricular (V) channel. On the marker channel, many of the low-amplitude atrial signals are under-sensed, leading to failure to detect atrial arrhythmias. In addition, current clinical practice guidelines for the treatment of device-detected atrial high-rate episodes are lacking. However, different trials used different definitions of an atrial high-rate event. Shorter cutoffs can lead to over-detection, commonly due to far-field R- and T-wave oversensing. Inspection of device-stored electrograms (and not only marker channels) is important to verify the accuracy of the device diagnostics. False-positive detections are often caused by noise oversensing, frequent atrial or ventricular premature beats, T-wave oversensing, or sinus arrhythmia. In fact, a large proportion (more than 60%) of patients are classified as having intermediate risk. Prior history of stroke, transient ischemic attack, or thromboembolism, age, gender, ethnicity, hypertension, diabetes, coronary artery disease, peripheral artery disease, cardiomyopathy, and heart failure are important risk factors. The stroke rate per 100 patientyears without antithrombotic therapy increases by a factor of approximately 1. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach. For each predictor, read the points assigned on the 010 scale at the top and then sum these points. Find the number on the "Total Points" scale and then read the corresponding predictions of 1- and 3-year risk of stroke or systemic embolism below it. Bleeding Risk Stratification Oral anticoagulation is associated with increased risk of bleeding. Therefore an assessment of bleeding risk should be part of the patient assessment before starting anticoagulation. The risk of bleeding should be weighed against the potential benefit of stroke prevention in individual patients considered for anticoagulation therapy. Several risk models have been proposed to predict bleeding risk on antithrombotic therapy. Abnormal kidney function is defined as the presence of long-term dialysis or renal transplantation or serum creatinine concentration of at least 200 µmol/L. Bleeding refers to previous bleeding history or predisposition to bleeding, or both. It is important to understand that bleeding risk assessment is not a static phenomenon, and many common clinical factors that increase bleeding risk are potentially reversible. Further, a high bleeding risk score is not a reason to withhold anticoagulation therapy as such patients can potentially derive even greater net clinical benefit while on oral anticoagulation therapy. Instead, a high score should prompt careful review and follow-up as well as aggressive efforts at amelioration of potentially reversible bleeding risk factors. A careful history results in a well-planned focused work-up that serves as an effective guide to therapy. Examination can also disclose associated valvular heart disease, myocardial abnormalities, or heart failure. For control of symptoms, a safety-driven approach is of paramount importance because most treatments (drug, surgery, ablation) have the capacity to produce significant morbidity and even mortality. Laboratory Testing Laboratory evaluation includes assessment of serum electrolytes, renal, and hepatic function, and a blood count. Aspirin is associated with only modest (22%) reduction in the incidence of stroke, corresponding to an absolute stroke risk reduction of 1. Thus except in the lowest risk patients, aspirin alone is not a viable treatment option for stroke prevention. The combination of aspirin plus clopidogrel is superior to aspirin therapy alone (28% relative risk reduction), but it is associated with a significantly increased risk of major bleeding (2.
Shortening of telomeres (nucleoprotein complexes protecting the chromosome ends that are involved in chromosome stability and repair) has been associated with an inflammatory phenotype and increased mortality in dialysis patients arthritis in back of neck order 75 mg indomethacin amex. It has also been speculated that biofilm formation is a cause of inflammation in this patient group. This relation is illustrated by the fact that alleviating inflammation reduces peritoneal angiogenesis. In addition, glucose-based solutions lead to a substantial uptake of glucose, which may be associated with the induction of oxidative stress, dyslipidemia, and malnutrition, all of which are potent causes of inflammation. Patients presenting high peritoneal solute transport rates have worse clinical conditions, characterized by worse nutritional status and enhanced inflammation. Moreover, an indwelling catheter potentiates inflammatory response through a foreign body reaction. Indeed, there are several factors specific of the dialysis technique that are widely accepted as contributors to inflammation. Although interestingly, dialysis-related inflammation seems to be associated with a specific genomic pattern,82 several in vivo studies suggest that the membrane composition, the type and quality of dialysis, and the type of vascular access may contribute to inflammatory processes. Cytokine production may be triggered by substances present in the dialysis fluid, which may penetrate intact dialyzer membranes. The type of vascular access has an important effect on inflammatory status and further outcomes. Mice lacking the gene encoding for fetuin-A rapidly develop ectopic soft tissue ossification and die at an early age. Some possible mechanisms have been proposed, including reduced iron availability and deterioration in the red cell line. Erythroid progenitors require coordination of iron acquisition and cell proliferation in the consecutive stages of maturation. In a pathway controlled by hepcidin, inflammation compromises the availability of iron for heme synthesis and, in consequence, impairs erythropoiesis. Due to increased hepcidin Endocrine Disorders the uremic state is associated with abnormalities of the endocrine system, affecting hormone production, metabolism, feedback regulation, and altered target tissue sensitivity. Evidence suggests that the observed hormonal dysmetabolism may be aggravated by persistent inflammation. This question does not yet have a clear answer; however, some studies have reported worse outcomes associated to these hormonal derangements, suggesting that it is not a completely physiological process. In fact, previous studies have connected the state of subclinical hypothyroidism with low-grade persistent inflammation. Although the high prevalence of hypogonadism observed in this group of patients to a great extent might be a consequence of the failing kidney per se,168 inflammation might have an important role in its physiopathology because it is known that inflammatory cytokines have a suppressive effect on the hypothalamicpituitarytesticular axis. This protective mechanism, ensuring a sustained energy flow in acute inflammation, becomes debilitating in chronic and persistent conditions of immune stimulation. The attrition of telomeres-the repetitive regions located at the end of chromosomes-is postulated to be a surrogate marker of cell senescence. What is true is that despite many markers having been studied and suggested, only very few of them meet requirements that make them appropriate for use in clinical practice. Unlike what happens in the general population, in whom consensus has been made in terms of the established cut-off values for diagnosis of inflammation. Some years ago, based on published data from pooled European cohorts, a cut-off point of 10 mg/L was proposed to define uremia-related inflammation,5 and this value has become the most frequently used cut-off point in clinical research for the prediction of outcome. The search for the perfect marker is complicated in patients with kidney disease, in whom some basic inflammatory markers. It is produced mainly by activated macrophages, although many other cell types can produce it. Among commonly available biomarkers (which will not be further discussed here), white blood cell count and immunocompetent cells, including leukocytes, monocytes, and lymphocytes (see Table 14. In normal conditions, pentraxin is detected in blood in very low levels, although it increases rapidly after noxious triggers. Routine examination allows confining the area of investigation to the most probable sites of infection, helping plan the next laboratory and imaging steps, and deciding about the urgency of an observed complication. These- and many other biomarkers related to inflammation-reflect various specific aspects of inflammation that are relevant to its pathophysiology and downstream consequences. Approaching a Patient With Inflammation Regular assessment of inflammatory status is warranted in patients with advanced kidney failure. The most important step in this investigation remains a detailed medical history and thorough physical examination. The routine examination allows confining the area of investigation to the most probable sites of infection, helping plan the next laboratory and imaging steps, and deciding about the urgency of an observed complication. Attention should be directed to the vascular/peritoneal access in the first instance. In parallel, the volume status of the patient should be assessed and, especially, fluid overload excluded. Importantly, other laboratory indices should be analyzed, including persistent anemia, improper white blood cell and platelet counts, acid-base balance, parameters of dialysis adequacy, parameters of heart and muscle ischemia, coagulation, transaminases, and cultures. At this step, chest x-ray and abdominal ultrasound examination should be also performed if not attained earlier. Persistent anemia accompanying persistent inflammation in a patient with a vascular access should draw attention to suspicion of endocarditis, and performing echocardiography should be advocated. At this stage of investigation, it is also important to exclude the exacerbation of concomitant comorbidities, especially of rheumatologic origin. Nonfunctioning kidney grafts and vascular accesses should be screened and removed if indicated.
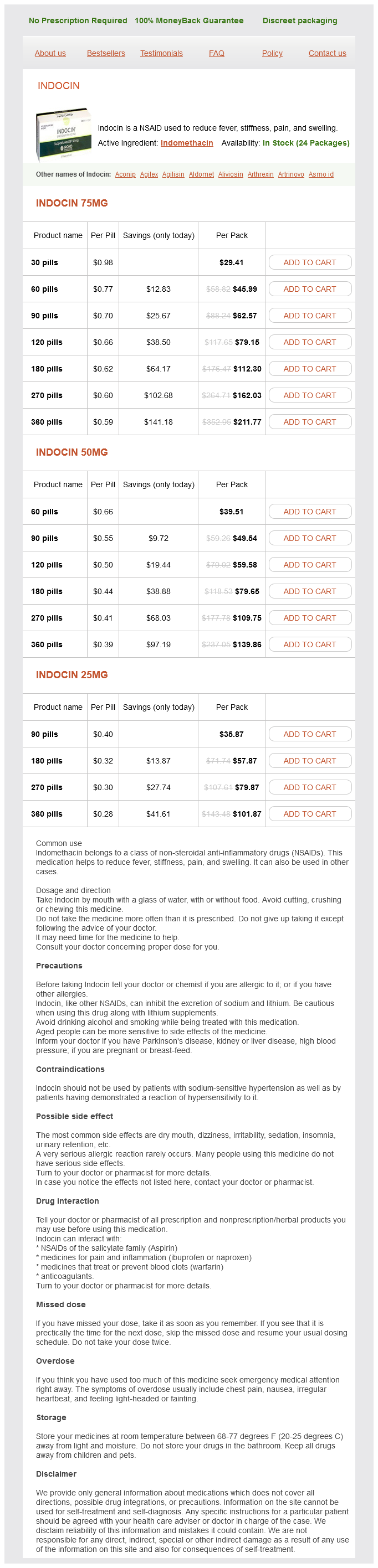
Indomethacin Dosage and Price
Indocin 75mg
- 30 pills - $29.41
- 60 pills - $45.99
- 90 pills - $62.57
- 120 pills - $79.15
- 180 pills - $112.30
- 270 pills - $162.03
- 360 pills - $211.77
Indocin 50mg
- 60 pills - $39.51
- 90 pills - $49.54
- 120 pills - $59.58
- 180 pills - $79.65
- 270 pills - $109.75
- 360 pills - $139.86
Indocin 25mg
- 90 pills - $35.87
- 180 pills - $57.87
- 270 pills - $79.87
- 360 pills - $101.87
Vitamin D insufficiency and effect of cholecalciferol in children with chronic kidney disease rheumatoid arthritis in the knee pictures buy generic indomethacin from india. Vitamin D insufficiency and hyperparathyroidism in children with chronic kidney disease. Vitamin D insufficiency and deficiency in children with early chronic kidney disease. Vitamin D deficiency and parathyroid hormone levels following renal transplantation in children. Decreased free 1,25-dihydroxycholecalciferol index in patients with the nephrotic syndrome. Vitamin D metabolites and calcium metabolism in patients with nephrotic syndrome and normal renal function. Vitamin D and calcium metabolism in children with nephrotic syndrome of normal renal function. Impact of kidney bone disease and its management on survival of patients on dialysis. Association of activated vitamin D treatment and mortality in chronic kidney disease. Vitamin D treatment and mortality in chronic kidney disease: a systematic review and meta-analysis. Vitamin D compounds for people with chronic kidney disease not requiring dialysis. Differentiation of mouse myeloid leukemia cells induced by 1 alpha,25-dihydroxyvitamin D3. Osteomalacia and hyperparathyroid bone disease in patients with nephrotic syndrome. Bone histology and calcium metabolism in patients with nephrotic syndrome and normal or reduced renal function. Absence of metabolic bone disease in adult patients with the nephrotic syndrome and normal renal function. Vitamin D in incident nephrotic syndrome: a Midwest Pediatric Nephrology Consortium study. Metabolic profiling of major vitamin D metabolites using Diels-Alder derivatization and ultra-performance liquid chromatography-tandem mass spectrometry. The vitamin D story: a collaborative effort of basic science and clinical medicine. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Prostate cancer risk and prediagnostic serum 25-hydroxyvitamin D levels (Finland). Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. Calcitriol modulates in vivo and in vitro cytokine production: a role for intracellular calcium. Quantification of pancreatic beta cell sensitivity to glucose and tissue sensitivity to insulin. Body mass index and fat mass are the primary correlates of insulin resistance in nondiabetic stage 3-4 chronic kidney disease patients. Stimulation by 1,25-dihydroxyvitamin D3 of insulin receptor expression and insulin responsiveness for glucose transport in U-937 human promonocytic cells. Identification of a Vitamin D response element in the human insulin receptor gene promoter. Transcriptional activation of the human insulin receptor gene by 1,25dihydroxyvitamin D(3). Intravenous 1,25 dihydroxycholecalciferol corrects glucose intolerance in hemodialysis patients. Amelioration of hypertension and insulin resistance by 1,25-dihydroxycholecalciferol in hemodialysis patients. Effects of intravenous calcitriol on lipid profiles and glucose tolerance in uraemic patients with secondary hyperparathyroidism. Effect of oral calcitriol pulse therapy on the lipid, calcium, and glucose homeostasis of hemodialysispatients: its safety in a combination with oral calcium carbonate. Paricalcitol does not improve glucose metabolism in patients with stage 3-4 chronic kidney disease. The renin-angiotensin system in glomerular podocytes: mediator of glomerulosclerosis and link to hypertensive nephropathy. Effect of depot oral cholecalciferol treatment on secondary hyperparathyroidism in stage 3 and stage 4 chronic kidney diseases patients. Effects of long-term cholecalciferol supplementation on mineral metabolism and calciotropic hormones in chronic kidney disease. Cholecalciferol (vitamin D3) therapy and vitamin D insufficiency in patients with chronic kidney disease: a randomized controlled pilot study. High-dose cholecalciferol to correct vitamin D deficiency in haemodialysis patients. Impact of ergocalciferol treatment of vitamin D deficiency on serum parathyroid hormone concentrations in chronic kidney disease. Prevalence of vitamin D deficiency and the safety and effectiveness of monthly ergocalciferol in hemodialysis patients. Vitamin D in chronic kidney disease: a systemic role for selective vitamin D receptor activation.
© 2025 Adrive Pharma, All Rights Reserved..