General Information about Ilosone
In conclusion, Ilosone is a useful medication in the struggle in opposition to bacterial infections. It is often used to treat respiratory and pores and skin infections and may also be used to prevent extra extreme infections. It is important to use this medication responsibly and solely as prescribed by a physician. With proper use, Ilosone can successfully treat infections and improve general well being and well-being.
Ilosone is usually well-tolerated and has been proven to be efficient in treating bacterial infections. It is essential to use this medication as directed and to complete the total course of remedy to make sure the absolute best outcomes. If symptoms don't improve or turn into worse, you will need to seek the guidance of with a well being care provider. In some circumstances, a special antibiotic may be essential for remedy.
In addition to treating infections, Ilosone can additionally be used to forestall certain bacterial infections. It is usually used to stop bacterial endocarditis, which is an infection of the lining of the guts or heart valves. This is particularly important for patients with coronary heart conditions or those undergoing dental or surgical procedures that may introduce bacteria into the bloodstream. Ilosone may also be used to stop rheumatic fever, a serious complication of strep throat.
The major use of Ilosone is to treat infections attributable to sure types of bacteria. It works by inhibiting the growth and replica of those micro organism, permitting the physique's immune system to battle off the an infection more effectively. This medication is most commonly used to treat respiratory tract infections, similar to pneumonia, bronchitis, and whooping cough. It may also be used to deal with skin infections, such as pimples and cellulitis.
Ilosone is on the market in various types, together with tablets, capsules, liquid, and topical solutions. The dosage and duration of treatment will vary depending on the kind and severity of the an infection. It is essential to follow the prescribed dosage and end the whole course of remedy, even if symptoms enhance, to make sure full recovery and prevent the bacteria from developing resistance.
Ilosone, also recognized as erythromycin, is a generally prescribed antibiotic used to deal with varied bacterial infections. This powerful treatment is effective against a variety of bacteria and has been confirmed to be a dependable therapy choice for lots of sufferers.
In some cases, Ilosone could also be used for different purposes, as prescribed by a doctor. This could embrace treatment for circumstances similar to chlamydia, syphilis, and pelvic inflammatory disease. It may also be used in combination with different medications to treat more extreme or difficult infections.
As with any medicine, there are some potential unwanted effects related to Ilosone. These can vary from mild effects, such as nausea and vomiting, to more severe reactions, similar to severe allergic reactions. It is important to tell the prescribing physician of any allergic reactions or different medical circumstances earlier than starting treatment with Ilosone.
It is important to note that Ilosone is only effective in opposition to bacterial infections and will not work for viral infections, such as the widespread chilly or flu. Using antibiotics unnecessarily can result in antibiotic resistance, making it tough to deal with infections in the future. Therefore, you will want to at all times consult with a well being care provider before taking Ilosone or some other antibiotic.
On cross sectioning medicine versed order ilosone 250 mg with amex, their lumina are narrowed because of prominent fibrotic plaques and atheromas. In acute occlusion, the plaques rupture and the defect in the endothelium is covered with a clot occluding the narrowed lumen. In older lesions, such thrombi are partially organized by granulation tissue that has grown into them from the vessel wall. Some thrombi appear to be recanalized, that is, traversed by numerous small blood vessels that have reestablished blood flow across the occluded segment of the artery. An infarct is characterized by ischemic cell death, which can be recognized morphologically first by typical microscopic changes and then by macroscopic changes in the heart. The first light microscopic changes occur approximately 24 hours after the onset of occlusion. Thereafter, cross sections of the heart show that fibrosis predominates; old infarcts appear as whitish gray, firm, and irregularly shaped scars that are slightly depressed and easily distinguishable from the brown color of normal myocardium. The endocardium overlying the infarcted myocardium is often damaged and disrupted. The blood within the ventricle coagulates in contact with the necrotic endocardium or the exposed myocardium and forms a thrombus attached to the wall of the ventricle. Such thrombi impede the blood flow and weaken the contraction of the ventricular myocardium, which may contribute to heart failure. Furthermore, fragments of the thrombus may detach, giving rise to emboli, which can cause infarcts in distant organs. Cerebral infarcts caused by such emboli are an important complication of myocardial infarcts. Softened necrotic myocardium may rupture as a result of the increased pressure of the blood within the ventricle. This compression of the heart by blood in the pericardial cavity typically occurs as a complication of ventricular rupture 5 to 7 days after infarction and usually is lethal. Massive myocardial infarcts of the left ventricle, which are replaced by fibrous scars, bulge under the pressure of blood in the left ventricle, forming an aneurysm. The heart is dilated and contracts irregularly because the fibrous scar forming the wall of the aneurysm does not contain contractile elements. Macrophages persist in the lesion for some time, during which they phagocytize and remove the necrotic myocardial cells and help in the formation of granulation tissue that begins to appear toward the end of the first week. As in wound healing, granulation tissue is composed of small blood vessels, myofibroblasts, and fibroblasts depositing extracellular matrix. In older infarcts, fibroblasts predominate, the collagenous matrix is more prominent, and small blood vessels are less prominent. On gross examination, the infarcted area cannot be definitively identified during the first 1 to 2 days. Approximately 3 to 5 days after the occlusion, the infarct becomes yellow and is surrounded by a hemorrhagic rim. The yellow infarcted myocardium is softened as a result of the action of hydrolytic enzymes released from the leukocytes. The most important clinical presentations of coronary heart disease are the following: · Congestive heart failure · Angina pectoris · Myocardial infarct Congestive heart failure Most of the symptoms of coronary heart disease are a consequence of hypoxia of the myocardium, which results in pump failure. The enlarged liver stretches the capsule, and this stimulates the nerves in the capsule, causing pain below the right costal margin. In addition, pressure in the abdominal veins may lead to the accumulation of fluid in the abdominal cavity. Failure of the left ventricle leads to pulmonary congestion and pulmonary edema, secondary to transudation of fluids into the alveoli. In milder cases, dyspnea develops only when the patient exercises or works strenuously. Because of a lack of oxygen, brain functions are slowed, and patients become somnolent, cannot concentrate, and easily develop mental fatigue. Hypoperfusion of the kidneys results in a reduction of urine formation (oliguria). Renal failure causes retention of sodium and water, which results in generalized edema. Lung insufficiency presents as pulmonary edema and acute respiratory distress syndrome. This additional effort cannot be sustained because the narrowed blood vessels do not allow influx of blood into the myocardium. The resulting ischemia causes pain, which is called angina pectoris, the Latin term for "chest pain. However, as the atherosclerosis progresses, nitroglycerin becomes less and less efficient. In most cases this is a consequence of major arrhythmia, including ventricular fibrillation, heart block, or asystole (cardiac arrest) with subsequent pump failure. Patients typically experience crushing precordial pain, often followed by loss of consciousness or fainting. By the time the infarct is recognized, the patient is prostrate, without a pulse, and in severe distress. Unless cardiothoracic resuscitation is initiated immediately, death may occur within minutes. Even with closed chest cardiac massage, mouth-to-mouth resuscitation and timely defibrillation (electric shock treatment) to restart the heart has poor results if the asystole (no systolic contractions) has lasted a few minutes.
To accomplish these three goals 97110 treatment code buy ilosone canada, basic screening laboratory tests including complete blood count, chemistry profile, erythrocyte sedimentation rate, electrolytes, serum thyroxine, and antinuclear antibody testing should be obtained. Magnetic resonance imaging of the head and spine with and without gadolinium will help rule out other central nervous system diseases that may mimic post-polio syndrome (see later). Electromyography is highly specific in the diagnosis of anterior horn cell disease, although the test can be suggestive but not specific for polio. Treatment of post-polio syndrome is aimed primarily at maximizing function and the relief of symptoms. Physical and occupational therapy to maintain and improve function is the cornerstone of the management of post-polio syndrome. Respiratory and speech therapy is indicated if swallowing, sleep, and/or breathing problems are present. The pain of post-polio syndrome is managed with simple analgesics, anti-inflammatory agents, topical analgesic balms, and moist heat. Weakness can be managed pharmacologically with anticholinesterase agents such as pyridostigmine (Mestinon). Failure to treat post-polio syndrome may result in loss of functional ability, an increased risk of falls due to muscle weakness, dehydration and malnutrition secondary to swallowing abnormalities, and recurrent respiratory infections due to diaphragmatic weakness. Inactivity associated with post-polio syndrome may increase the risk of osteoporosis. Diseases that need to be considered in the differential diagnosis of postpolio syndrome are outlined in Table 213-2. Given the implications of missing the diagnosis of many of the diseases listed in Table 213-2, postpolio syndrome must be considered a diagnosis of exclusion. Suggested Readings Boukara Z, Bedjaoui M, Bensaber O, Ammor S, Talbi A, Tou S, Lahmer A: Spinal pain and post poliomyelitis syndrome, Ann Phys Rehabil Med, 54(1):e267e268, 2011 Oct. As the weakness and sensory dysfunction ascend, respiratory difficulties combined with paralysis of the lower cranial nerves may occur. The evolution phase is the period of time from onset of symptoms to the nadir of symptoms. The plateau phase begins at the nadir of symptoms and continues until the clinical recovery phase begins. The plateau phase on average can last for 2 to 4 weeks before the clinical recovery phase begins. The clinical recovery phase takes place over a period of many weeks, with most patients experiencing significant recovery within 25 to 30 weeks. The remaining 15% may suffer from permanent residual neurologic defects including footdrop, weakness, and the like. Bacteria that have been implicated include Campylobacter, Haemophilus influenzae, and Borrelia burgdorferi, among others. Mycoplasma pneumoniae and Epstein-Barr virus, cytomegalovirus, and Zika virus have also been implicated. Finding on cerebrospinal fluid analysis includes elevated protein with normal cerebrospinal fluid cell counts. Aggressive management of impending respiratory insufficiency with endotracheal intubation and mechanical intubation should be considered sooner rather than later given the progressive nature of the disease. Aggressive physical and occupational therapy to maintain function should be an integral part of the treatment plan. Pain should be managed with simple analgesics and nonsteroidal anti-inflammatory drugs, with narcotics being reserved for acute exacerbations or incident-related pain. These changes in the shape of the red blood cell usually take the form of a sickle shape and are due to aggregation of the hemoglobin protein. If this process continues unabated, tissue ischemia and ultimately infarction may occur. These ischemic episodes are called vaso-occlusive or sickle cell crises, and they occur intermittently and are associated with significant morbidity and, rarely, mortality. Although all organs are at risk for damage from vaso-occlusive crises, the long bones and spleen are particularly susceptible to damage. In many patients with more severe forms of sickle cell disease the spleen can suffer complete infarction, resulting in an autosplenectomy. Other serious complications associated with sickle cell disease include aplastic crises and splenic sequestration crises. A rapidly decreasing reticulocyte count is highly suggestive of aplastic crises in this clinical setting. Splenic sequestration crisis is manifested clinically as an acutely painful enlargement of the spleen. These complications of sickle cell disease mentioned can act either alone or in combination to produce significant morbidity for patients suffering from this serious disease (Table 215-1). More common problems caused by these complications include hyposplenism-associated infections, stroke, cholelithiasis, osteomyelitis, retinopathy, and nephropathy. Sickle cell disease occurs most commonly in individuals whose ancestors hailed from sub-Saharan Africa, the Middle East, India, and the Mediterranean. The predilection for this region is thought to be the result of natural selection because although sickle cell disease is associated with a shortened life expectancy of 40 to 50 years, the presence of sickle cell hemoglobin confers resistance to malaria, which was a leading cause of death in this geographic region. In general, the pain associated with milder vaso-occlusive crises should be treated with simple analgesics and/or nonsteroidal anti-inflammatory drugs and oxygen. More severe pain Chapter 216 Dependence, Tolerance, and Addiction 343 may require opioid analgesics, although the risks of chemical dependence and addiction are high in this patient population owing to the recurring nature of the crises. The administration of zinc may help stabilize the red blood cell membrane, and the administration of hydroxyurea to increase the production of fetal hemoglobin in place of sickle hemoglobin can be considered. Suggested Readings Kesse-Adu R, Howard J: Inherited anaemias: sickle cell and thalassaemia, Medicine, 41(4):219224, April 2013. Perhaps in no other area of medicine has the lack of clarity and consistency in word usage done more damage to the understanding of disease and the care of patients.
Ilosone Dosage and Price
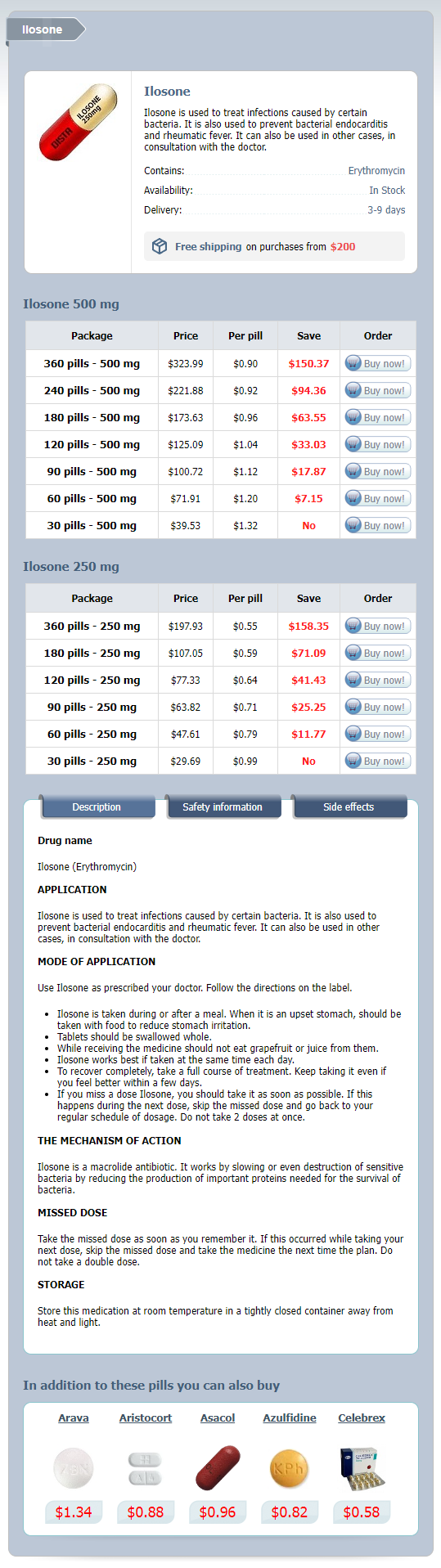
Ilosone 500 mg
- 360 pills - $323.99
- 240 pills - $221.88
- 180 pills - $173.63
- 120 pills - $125.09
- 90 pills - $100.72
- 60 pills - $71.91
- 30 pills - $39.53
Ilosone 250 mg
- 360 pills - $197.93
- 180 pills - $107.05
- 120 pills - $77.33
- 90 pills - $63.82
- 60 pills - $47.61
- 30 pills - $29.69
In some cases medications while pregnant discount 250mg ilosone mastercard, it is thought that humans auto-infect with the contaminated eggs of their own tapeworm. Cysticercus development is coincident with modulation of host immune responses, favoring expression of parasite immune evasion mechanisms that interfere with Th2type protective immune responses. Dying parasites release their suppressive hold on protective host immune responses, and antigens are released. When cellular reactions are present, they are in part due to the result of interleukin signaling from T cells. This environment is frequently contaminated with human feces in many regions of the world where pigs are raised. Patients are usually asymptomatic, and do not become aware of their infection until they discover the proglottids in stool, on the perianal skin, in clothing, or bed sheets. Some patients report abdominal pain, distension, diarrhea, and nausea, but there are no controlled studies to demonstrate their link with the presence of T. There may be geographic variation in this clinical presentation because subcutaneous cysticercosis is common in Asia and Africa, but rare in Latin America. Some patients with extraneural cysticercosis can also harbor cardiac cysticerci, which is usually also asymptomatic. Subsequent development of uveitis, retinitis, or choroidal atrophy can lead to visual loss. There appear to be geographic differences in the presentation of clinical neurocysticercosis. Gravid proglottid segments should be fixed in 10% formaldehyde solution, and injected with India ink to fill the uterus. These proglottid segments can also be prepared and viewed using standard hematoxylin and eosin staining. Polyethylene glycol salt purges to improve bowel cleaning significantly improves the likelihood of scolex recovery, but is not often used. Diagnosis of cysticercosis is usually based on imaging tests and criteria have been established. Because it is often not practical to biopsy cysticerci, consulting a neuroradiologist is extremely helpful. Praziquantel is usually available in developing countries, particularly because of its use for global schistosomiasis control, and its proven success in Mexico in reducing the prevalence where taeniasis is endemic. Radiogram of brain with calcified lesion due to infection with the metacestode of T. Serological testing assays have improved, with a sensitivity of 98 percent and a specificity approaching 100 percent. Taenia solium 349 (vesicular stage), degenerate (the colloidal stage), collapsed (granular nodular stage), or nonviable (calcified). Seizures most often occur in neurocysticercosis when the host inflammatory response is activated as parasites begin to die. In this situation, initiation of therapy can trigger edema with resultant seizure activity. Typically, this might include an infectious disease specialist, a neurologist, a neuroradiologist, an ophthalmologist and a neurosurgeon. The current recommendation is that therapeutic decisions on using albendazole (15 mg/kg daily for 10-14 days) with or without praziquantel (50mg/kg for 10 days) need to be tailored to the individual patient, based on the number, location, and viability of the cysticerci. Dexamethasone affects the blood levels of both praziquantel and albendazole, so drug doses of both may need to be adjusted. Neurosurgical management with placement of ventricular shunts is often required for complicated neurocysticercosis involving cerebrospinal obstruction and hydrocephalus. Prevention and Control Taenia solium is a significant public health problem, even outside the endemic areas, due to the association of cysticercosis with the adult infections. Individual infection is prevented by thoroughly cooking pork, or by freezing it at -10 °C for a minimum of 5 days. Community-based interventions comprised of sanitation and pig management highly effective in disease control. Some black bears in California have acquired cysticercosis, most likely as the result of feeding at garbage dumps near campgrounds. Hunter organizations should issue warnings, advising hunters that any meat obtained from carnivores or omnivores should be cooked well before eating. Fifty Sixth World Health Organization, Control of neurocysticercosis, Report by the Health Assembly. Diphyllobothrium latum (Linnaeus 1758) Introduction Diphyllobothrium latum belongs to the order Pseudophyllidea and usually achieves a length of 2-15 meters, but has achieved a length of 25 meters, making it the longest parasite to infect humans. It has a unique affinity for absorbing vitamin B12, and as a result the infection can have pathological consequences for some infected individuals. Diphyllobothrium pacificum), has been reported from the Most carnivores are susceptible to infection Pacific Coast of South America - Peru, Chile, with D. Some cies in the region (possibly linked to ceviche of these hosts are important reservoirs for the consumption). It is still common throughout Descriptions of what appears to have been Scandinavia, though prevalence in that region infection due to the broad or fish tapeworm has decreased in recent years due in large part, go back thousands of years, with archaeologito vastly improved sanitation. In the northern hemisphere, pike and percids are the most common source of infection in many regions of the world. The plerocercoid larvae, now free of fish muscle, pass to the small intestine and attach to the intestinal wall by applying their two bothria (grooves) to the epithelial surface.
© 2025 Adrive Pharma, All Rights Reserved..