General Information about Hytrin
It is vital to inform a doctor about any pre-existing medical conditions or allergies earlier than starting Hytrin treatment. This consists of any history of low blood stress, liver or kidney disease, or a personal or household history of prostate most cancers. Pregnant or breastfeeding women must also avoid taking Hytrin, as its effects on the creating fetus or infant are unknown.
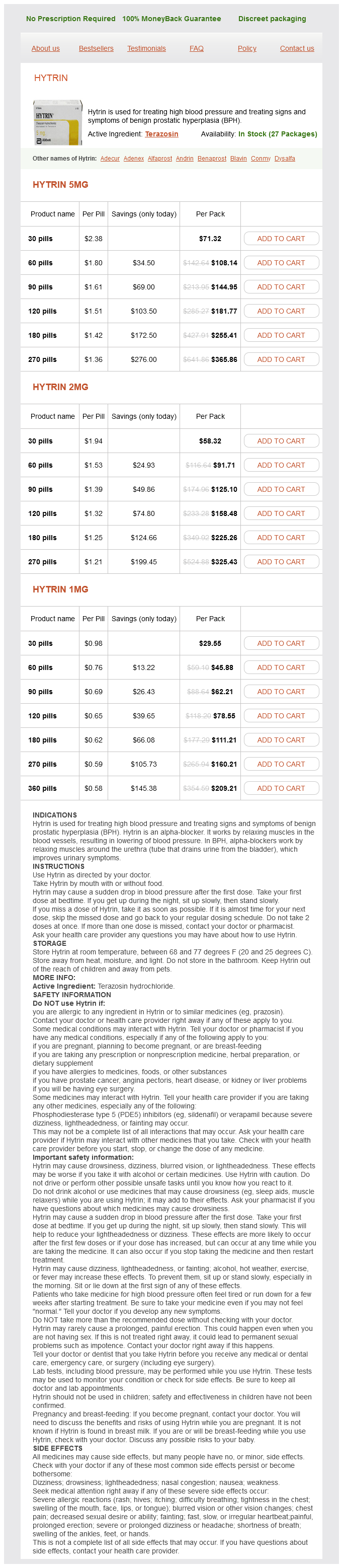
Hytrin, also referred to as terazosin, is a medicine that is commonly prescribed for 2 major purposes – treating high blood pressure and treating indicators and symptoms of benign prostatic hyperplasia (BPH). This drug belongs to a class of medications called alpha-1 blockers, which work by enjoyable the muscular tissues within the blood vessels and the prostate, allowing for an enchancment in blood circulate and a discount in signs associated with BPH.
BPH, then again, is a non-cancerous situation that affects the prostate gland, which is located in males and plays a job in the reproductive system. As men age, the prostate gland can develop in measurement, leading to the event of BPH. This may cause symptoms corresponding to frequent and pressing urination, difficulty urinating, and a weak or interrupted urine stream. By stress-free the muscular tissues within the prostate, Hytrin may help alleviate these signs and improve the quality of life for those affected by BPH.
Hytrin is available in pill kind and is normally taken once day by day. The dosage could range depending on the person's medical condition and response to therapy, and should always be prescribed and monitored by a healthcare professional. It is essential to follow the prescribed dosage and not to stop taking Hytrin abruptly without consulting a doctor, as this could trigger a sudden improve in blood strain.
High blood strain, also referred to as hypertension, is a common medical situation that impacts hundreds of thousands of people worldwide. It happens when the pressure of blood in opposition to the partitions of the arteries is just too high, which can lead to serious well being problems similar to coronary heart illness, stroke, and kidney disease. Hytrin works by dilating the blood vessels, making it simpler for blood to move and decreasing the general blood pressure. This can effectively decrease the chance of potential problems associated with hypertension.
As with any medicine, Hytrin could trigger some unwanted facet effects in sure individuals. Some frequent unwanted effects embody dizziness, headache, fatigue, and nausea. It is essential to tell a physician if these unwanted effects persist or turn out to be more extreme. In rare instances, Hytrin may cause a sudden drop in blood pressure, particularly when starting treatment or increasing the dosage. This is more more doubtless to occur in people who're also taking different blood pressure medications.
In conclusion, Hytrin is a extensively prescribed medicine for treating high blood pressure and BPH. It works by dilating blood vessels to improve blood circulate and relaxing the muscular tissues in the prostate to reduce symptoms of BPH. As with any medicine, it is essential to comply with the prescribed dosage and seek the assistance of a well being care provider if any side effects happen. With proper use and monitoring, Hytrin can help enhance high quality of life and reduce the danger of potential issues related to high blood pressure and BPH.
One obvious difference between them is that graded potentials function only in short-distance communication blood pressure chart hypertension buy genuine hytrin on line, but the propagation of action potentials permits communication over long distances. Our focus in this chapter is on synaptic communication among the billions of neurons in the nervous system. Some diseases and neurological disorders result from disruptions of synaptic transmission. Synapses also are the sites of action for many therapeutic and addictive chemicals. The two types of synapses, chemical and electrical, differ both structurally and functionally. Arrows indicate the direction of information flow: presynaptic neuron n postsynaptic neuron. Presynaptic neurons usually synapse on the axon (axoaxonic; red), a dendrite (axodendritic; blue), or the cell body (axosomatic; green). In a chemical synapse, an impulse in a presynaptic neuron causes the release if neurotransmitter molecules that produce an impulse in a postsynaptic neuron. Although the plasma membranes of presynaptic and postsynaptic neurons are in close proximity at a chemical synapse, their plasma membranes do not touch. Because impulses cannot conduct across the synaptic cleft, an alternative, indirect form of communication occurs between the presynaptic and postsynaptic neurons. In response to an impulse, the presynaptic neuron releases neurotransmitter molecules that diffuse through the fluid in the synaptic cleft and bind to receptors in the plasma membrane of the postsynaptic neuron. The postsynaptic neuron receives the chemical signal and, in turn, produces a postsynaptic potential, a type of graded potential. Thus, the presynaptic neuron converts an electrical signal (impulse) in to a chemical signal (released neurotransmitter). The postsynaptic neuron receives the chemical signal and, in turn, generates an electrical signal (postsynaptic potential). The time required for these processes at a chemical synapse, a synaptic delay of about 0. The depolarizing phase of the impulse opens voltage-gated Ca2 channels in the membrane of synaptic end bulbs. Because calcium ions are more concentrated in the extracellular fluid, Ca2 flows inward through the opened channels. An increase in the concentration of Ca2 inside the presynaptic neuron triggers exocytosis of some of the synaptic vesicles. Through exocytosis of synaptic vesicles, a presynaptic neuron releases neurotransmitter molecules. After diffusing across the synaptic cleft, the neurotransmitter binds to receptors in the plasma membrane of the postsynaptic neuron and produces a postsynaptic potential. The postsynaptic neuron then converts the chemical signal back in to an electrical signal (postsynaptic potential). Synchronizing action potentials in the heart or in visceral smooth muscle coordinates contractions to produce a heartbeat or move food through the gastrointestinal tract. Binding of neurotransmitter molecules to their receptors on ligand-gated channels opens the channels and allows particular ions to flow across the membrane. As ions flow through the opened channels, the voltage across the membrane changes. Depending on which ions the channels admit, the postsynaptic potential may be a depolarization (excitation) or hyperpolarization (inhibition). For example, opening of Na channels allows inflow of Na, which causes depolarization. When a depolarizing postsynaptic potential reaches threshold, it triggers an action potential in the axon of the postsynaptic neuron. Excitatory and Inhibitory Postsynaptic Potentials A neurotransmitter causes either an excitatory or an inhibitory graded potential. During hyperpolarization, generation of an action potential is more difficult than usual because the membrane potential is more negative and thus even farther from threshold than in its resting state. For example, synaptic transmission at a neuromuscular junction proceeds from a motor neuron to a skeletal muscle fiber (but not in the opposite direction). Integration of these inputs involves summation of the postsynaptic potentials that form in the postsynaptic neuron. If the total excitatory effects are greater than the total inhibitory effects and threshold is reached, one or more action potentials will be triggered. The result is inhibition of the postsynaptic neuron and an inability to generate an action potential. Electrical Synapses In an electrical synapse, impulses conduct directly between the plasma membranes of adjacent neurons through gap junctions. As ions flow from one cell to the next through these tunnel-like structures, the impulse spreads from cell to cell. As ions flow from one cell to the next through the gap junctions, the action potential spreads from cell to cell. Gap junctions are common in visceral smooth muscle, cardiac muscle, and the brain. Because action potentials conduct directly through gap junctions, electrical synapses are faster than chemical synapses. At an electrical synapse, the action potential passes directly from the presynaptic cell to the postsynaptic cell.
The second group of sympathetic ganglia blood pressure chart when to go to the hospital cheap hytrin 2 mg visa, the prevertebral ganglia, lies in the abdomen and anterior to the vertebral column. In general, postganglionic axons from prevertebral ganglia innervate organs below the diaphragm. Preganglionic neurons of the parasympathetic division synapse with postganglionic neurons in terminal ganglia. Because terminal ganglia are located either close to or in the wall of the visceral organ, parasympathetic preganglionic axons are long, in contrast to parasympathetic postganglionic axons, which are short. An axon may continue, without synapsing, through the sympathetic trunk ganglion to end at a prevertebral ganglion where it synapses with postganglionic neurons. Axons leave the sympathetic trunk in three possible ways: (1) They can enter spinal nerves; (2) they can form sympathetic nerves; and (3) they can form splanchnic nerves. The chromaffin cells release hormones in to the blood that intensify responses elicited by sympathetic postganglionic axons. A single sympathetic preganglionic fiber has many axon collaterals (branches) and may synapse with 20 or more postganglionic neurons. This pattern of projection is an example of divergence and helps explain why many sympathetic responses affect almost the entire body simultaneously. In the terminal ganglion, the presynaptic neuron usually synapses with only four or five postsynaptic neurons, all of which supply a single visceral effector, allowing parasympathetic responses to be localized to a single effector. The major plexuses in the thorax are the cardiac plexus, which supplies the heart, and the pulmonary plexus, which supplies the bronchial tree. Located along the abdominal aorta are several autonomic plexuses; often the plexuses that innervate abdominal viscera are named after the artery along which they are distributed. The preganglionic axons of both the cranial nerves and sacral spinal nerves end in terminal ganglia, where they synapse with postganglionic neurons. The cranial parasympathetic axons have ganglia that innervate structures in the head and are located close to the organs they innervate. Preganglionic axons that leave the brain as part of the vagus (X) nerves extend to many terminal ganglia in the thorax to provide parasympathetic innervation to the heart and lungs, and to the abdomen to supply the liver, gallbladder, stomach, pancreas, small intestine, and part of the large intestine. Pelvic splanchnic nerves synapse with parasympathetic postganglionic neurons located in terminal ganglia in the walls of the innervated viscera. From the terminal ganglia, parasympathetic postganglionic axons innervate smooth muscle and glands in the walls of the colon, ureters, urinary bladder, and reproductive organs. Although this gastrointestinal environment is inside the body, it is still considered part of the external environment. Just as the surface of the body must respond to important environmental stimuli in order to function properly, the surface of the gastrointestinal tract must respond to surrounding stimuli to generate proper homeostatic controls. In fact, these responses and controls are so important that the gastrointestinal tract has its own nervous system with intrinsic input, processing, and output. The enteric nervous system can and does function independent of central nervous system activity, but can also receive controlling input from the central nervous system. The enteric nervous system is the specialized network of nerves and ganglia forming a complex, integrated neuronal network within the wall of the gastrointestinal tract, pancreas, and gallbladder. This incredible nerve network contains in the neighborhood of 100 million neurons, approximately the same number as the spinal cord, and is capable of continued function without input from the central nervous system. The enteric network of nerves and ganglia contains sensory neurons capable of monitoring tension in the intestinal wall and accessing the composition of the intestinal contents. These sensory neurons relay their input signals to interneurons within the enteric ganglia. The interneurons establish an integrative network that processes the incoming signals and generates regulatory output signals to motor neurons throughout plexuses within the wall of the digestive organs. The motor neurons carry the output signals to the smooth muscle and glands of the gastrointestinal tract to exert control over its motility (movement) and secretory activities. Most of the nerve fibers that innervate the digestive organs arise from two plexuses within the enteric nervous system. The myenteric plexus communicates extensively with a somewhat smaller plexus, the submucous plexus, which occupies the gut wall between the circular muscle layer and the muscularis mucosae (see Concept 23. Neurons emerge from the ganglia of these two plexuses to form smaller plexuses around blood vessels and within the muscle layers and mucosa of the gut wall. It is this system of nerves that makes possible the normal motility and secretory functions of the gastrointestinal tract. What is the functional difference between preganglionic and postganglionic neurons Contrast the locations of sympathetic trunk ganglia, prevertebral ganglia, and terminal ganglia. Cholinergic neurons include (1) all sympathetic and parasympathetic preganglionic neurons, (2) sympathetic postganglionic neurons that innervate most sweat Autonomic neurons release neurotransmitters at synapses between neurons (preganglionic to postganglionic) and at synapses between neurons and autonomic effectors. Based on the neurotransmitter they produce and release, autonomic neurons are classified as either cholinergic or adrenergic. Autonomic neurotransmitters exert their effects by binding to specific receptors located in the plasma membrane of a postsynaptic neuron or effector cell. It then diffuses across the synaptic cleft and binds with specific cholinergic receptors on the postsynaptic plasma membrane. The two types of cholinergic receptors are nicotinic receptors and muscarinic receptors. Because acetylcholine is quickly inactivated by the enzyme acetylcholinesterase, effects triggered by cholinergic neurons are brief. The condition is due to excessive sympathetic stimulation of smooth muscle in the arterioles of the digits and a heightened response to stimuli that cause vasoconstriction. When arterioles in the digits vasoconstrict in response to sympathetic stimulation, blood flow is greatly diminished. As a result, the digits may blanch (look white due to blockage of blood flow) or become cyanotic (look blue due to deoxygenated blood in capillaries).
Hytrin Dosage and Price
Hytrin 5mg
- 30 pills - $71.32
- 60 pills - $108.14
- 90 pills - $144.95
- 120 pills - $181.77
- 180 pills - $255.41
- 270 pills - $365.86
Hytrin 2mg
- 30 pills - $58.32
- 60 pills - $91.71
- 90 pills - $125.10
- 120 pills - $158.48
- 180 pills - $225.26
- 270 pills - $325.43
Hytrin 1mg
- 30 pills - $29.55
- 60 pills - $45.88
- 90 pills - $62.21
- 120 pills - $78.55
- 180 pills - $111.21
- 270 pills - $160.21
- 360 pills - $209.21
With the exception of lymphocytes arteria femural order generic hytrin, formed elements do not divide once they leave red bone marrow. Myeloid and lymphoid stem cells give rise to precursor cells, also known as blasts. Over several cell divisions they develop in to the actual formed elements of blood. For example, monoblasts develop in to monocytes, eosinophilic myeloblasts develop in to eosinophils, and so on. Because erythrocytes have no nucleus, all of their internal space is available to transport oxygen molecules. A biconcave disc has a much greater surface area for the diffusion of gas molecules in to and out of the erythrocyte than, say, a sphere or a cube. A hemoglobin molecule consists of a protein called globin, composed of four polypeptide chains; a ringlike nonprotein pigment called a heme is bound to each of the four chains. Each oxygen molecule picked up from the lungs is transported bound to an iron ion within the heme ring. Essentially, erythrocytes consist of a plasma membrane enclosing a cytosol rich with hemoglobin. In (b), note that each of the four polypetide chains (blue) of a hemoglobin molecule has one heme group (gold), which contains an iron ion, Fe2 (shown in red). Hemoglobin also transports about 23 percent of the total carbon dioxide, a waste product of metabolism. As blood flows through the lungs, the carbon dioxide is released from hemoglobin and then exhaled (see Chapter 22). The plasma membrane becomes more fragile with age, and the cells are more likely to burst, especially as they squeeze through narrow channels in the spleen. Ruptured red blood cells are removed from circulation and destroyed by phagocytic macro- Macrophages in the spleen, liver, and red bone marrow phagocytize ruptured and worn-out red blood cells, splitting apart the globin and heme portions of hemoglobin. Globin is broken down in to amino acids, which can be reused by body cells to synthesize other proteins. Iron is needed for the heme portion of the hemoglobin molecule, and amino acids are needed for the globin portion. Within red bone marrow, erythropoiesis (red blood cell production) releases red blood cells in to the circulation. Within the liver, bilirubin is secreted by liver cells in to bile, which passes in to the small intestine and then in to the large intestine. As they traveled, they collided with red blood cells, white blood cells, and proteins. Thousands of transformed Plasmodium merozoites now burst forth from the liver and traveled in to the bloodstream. Normally, erythropoiesis and red blood cell destruction proceed at roughly the same pace. The controlled condition in this particular feedback loop is the amount of oxygen delivered to the kidneys (and thus to body tissues in general). For example, the lower oxygen content of air at high altitudes reduces the level of oxygen in the blood. Oxygen delivery may also decrease due to anemia, which can result from many causes; lack of iron, certain amino acids, and lack of vitamin B12 are but a few. Whatever the cause, hypoxia stimulates the kidneys to increase the release of the hormone erythropoietin. As you have already learned, the production of the formed elements of blood is called hemopoiesis. The proerythroblast divides several times, producing cells that begin to synthesize hemoglobin. Reticulocytes, which are about 34 percent hemoglobin and retain some mitochondria, ribosomes, and endoplasmic reticulum, pass from red bone marrow in to the bloodstream. Erythropoietin circulates through the blood to the red bone marrow, where it speeds the development of proerythroblasts in to reticulocytes. It then takes one to two days for the reticulocytes to lose the last vestiges of endoplasmic reticulum and become erythrocytes. A high "retic" count might indicate a good red bone marrow response to previous blood loss or to iron therapy in someone who had been irondeficient. A hematocrit indicates the percentage of the blood volume occupied by red blood cells. How might your hematocrit change if you moved from a town at sea level to a high mountain village where the air contains less oxygen Increased oxygen delivery to tissues the main stimulus for erythropoiesis is when kidney cells detect low oxygen levels in the blood. There are at least 24 blood groups, and more than 100 antigens that can be detected on the surface of red blood cells. The surfaces of erythrocytes contain a genetically determined assortment of antigens composed of glycoproteins and glycolipids. Based on the ¯ presence or absence of various antigens, blood is categorized in to different blood groups. Although agglutinins start to appear in the blood within a few months after birth, the reason for their presence is not clear. Perhaps they are formed in response to bacteria that normally inhabit the gastrointestinal tract. These are the anti-A antibody, which reacts with antigen A, and the anti-B antibody, which reacts with antigen B. A transfusion is most often given to alleviate anemia, to increase blood volume (for example, after a severe hemorrhage, the loss of a large amount of blood), or to improve immunity.
© 2025 Adrive Pharma, All Rights Reserved..