General Information about Celebrex
It is necessary to notice, nevertheless, that while Celebrex offers effective pain relief, it is not a cure for arthritis or some other condition. It merely supplies short-term relief and doesn't handle the underlying cause of the ache. Therefore, it should not be used as a long-term remedy option and should at all times be taken under the supervision of a healthcare skilled.
In conclusion, Celebrex is a generally used NSAID that provides effective reduction for acute pain caused by arthritis and menstruation. Its unique capability to focus on inflammation whereas also defending the stomach lining and stopping blood clotting makes it a safer various to other NSAIDs. However, as with all treatment, it is very important use it beneath the guidance of a healthcare professional and to listen to potential unwanted side effects.
Celebrex can be a most popular alternative for many individuals because of its comfort and ease of use. It is available in capsule kind, which can be taken a few times a day relying on the severity of ache and the individual's response to the treatment. Unlike other NSAIDs that may need to be taken multiple times a day, Celebrex's longer duration of action implies that it can provide continued reduction without the necessity for frequent dosing.
One of the primary benefits of Celebrex is its capability to target the COX-2 enzyme, which is answerable for inflammation and pain. Unlike its predecessor, Vioxx, which was pulled from the market within the early 2000s as a outcome of its link to an increased threat of coronary heart assault and stroke, Celebrex has been proven to be a safer various. This is as a outcome of it additionally inhibits COX-1, another enzyme that plays a task in blood clotting and defending the lining of the stomach. This balanced inhibition of each COX enzymes makes Celebrex much less prone to cause severe adverse results on the heart and abdomen.
Menstrual cramps, also called dysmenorrhea, may be debilitating for some ladies and may greatly impression their daily actions and productivity. Celebrex can be a generally used therapy option for this kind of acute pain. As with arthritis, it targets the COX enzymes to scale back the manufacturing of prostaglandins, which are liable for the uncomfortable symptoms associated with menstrual cramps.
For these affected by arthritis, whether or not it be osteoarthritis or rheumatoid arthritis, the ache, stiffness, and swelling can significantly impression daily activities and high quality of life. This is where Celebrex is obtainable in, providing aid and bettering general perform for those battling this continual disease.
Celebrex, additionally recognized by its generic name celecoxib, is a non-steroidal anti-inflammatory drug (NSAID) that is generally used to deal with acute pain caused by conditions corresponding to arthritis and menstruation. It is a prescription medicine that works by reducing the hormones within the body that trigger irritation and ache.
Like any treatment, Celebrex may trigger unwanted effects in some individuals. These can vary from mild to severe relying on the person's medical history and other drugs they could be taking. Some frequent unwanted effects include headache, dizziness, stomach upset, and pores and skin rash. More severe unwanted side effects, although uncommon, might embody allergic reactions, liver harm, and an elevated danger of coronary heart attack and stroke.
It is necessary to inform your physician of some other drugs or dietary supplements you are taking before beginning Celebrex, as it might work together with certain drugs. People with a historical past of heart illness, hypertension, or abdomen ulcers must also train warning and inform their doctor before starting this treatment.
Given the multiple variables that impact calciumephosphate solubility rheumatoid arthritis quizlet cheap celebrex 100 mg with visa, the use of simple equations to calculate calciumephosphate limits which do not consider all factors should be avoided. In the absence of formulation-specific emulsion stability data, it is recommended that a 2-in-1 admixture be compounded and a lipid be administered as a separate infusion. Adding medications without the above-proven data can lead to unnecessary patient risks and is generally only considered routinely safe for regular insulin and H2 receptor antagonists. Both are stable in 3-in-1 admixtures of various formulations and may be added without hesitation. These changes induce rapid onset hypophosphatemia, hypomagnesemia, and/or hypokalemia which can lead to cardiac and respiratory failure and death. With dextrose overfeeding, the excess dextrose causes hyperinsulinemia, which in turn enhances glucose conversion into fat within the liver. At signs of liver dysfunction, lipids can be further reduced while ensuring no deficiencies result. In adults, such a process is most likely unnecessary, especially if the patient is receiving carbohydrates through their oral diet. Clinical guidelines: nutrition support of hospitalized adult patients with obesity. Improved equations for predicting energy expenditure in patients: the ireton-jones equations. How accurate are resting energy expenditure prediction equations in obese trauma and burn patients Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Intradialytic parenteral nutrition in maintenance hemodialysis patients suffering from protein-energy wasting. Micronutrient supplementation in adult nutrition therapy: practical considerations. Refeeding syndrome: screening, incidence, and treatment during parenteral nutrition. Residency training is becoming a common method for pharmacists to advance their skills and knowledge following pharmacy school,1 allowing pharmacists to be increasingly involved throughout the medication use process. Participation on rounding teams has been shown to decrease adverse drug events, with the potential to reduce hospital length of stay. Pharmacists in these settings, like their counterparts in inpatient practices, can work closely with the medical team to devise and adjust short- and longterm therapy plans for a wide range of conditions. By managing medication dosing and monitoring, pharmacists have improved hypertension and diabetes control, improving the quality of life for patients. Community Pharmacy Practice Community pharmacy practice comprises the majority of licensed pharmacists, wherein pharmacists review the appropriateness of prescribed medications as part of the dispensing process for ambulatory patients. Also, various other cognitive clinical services can be performed that can be funded by the patient, health insurance, or government, depending on the country. Given their availability, many surveys of patient and physician perceptions of pharmacist roles and impact are driven by services provided by community pharmacists. Clinical interventions in community practice settings often focus on comprehensive medication use reviews and patient counseling to decrease polypharmacy, improve dosing, and improve patient adherence. These programs are collectively referred to as Medication Management Services, officially recognized in the United States by the Centers for Medicare and Medicaid Services as a reimbursable pharmacist-provided service in community pharmacies. Medication therapy management programs, which may include pharmacist prescribing, identify drug therapy problems (such as needing additional medication therapy to treat an established condition) leading to improved disease control, and cost savings for health systems. As such, how a pharmacist interacts with patients and medical teams, including the degree of autonomy granted, may differ by practice location. Prescriptive Authority As described previously, pharmacists have been shown to improve patient care quality. As their interventions rely on the knowledgeable use of medications, prescriptive authority is a natural progression for pharmacists with advanced training or demonstration of appropriate skills and knowledge. Decisions are mapped out in detail, and pharmacists assess clinical situations to determine which plan to implement. A broader application of clinical knowledge is used in collaborative practice, wherein a written agreement outlines criteria for patients the pharmacist may address, responsibilities of the pharmacist, training requirements for the pharmacist, and broad guidelines to ensure consistent care. Independent prescribing, as is available in some healthcare systems such as the United Kingdom, does not require prior agreements with physicians to permit assessment and treatment. Through privileging, the hospital can review the credentials of nonphysician clinicians and permit independent action within the scope of practice outlined by the state. Pharmacist Providers Although prescriptive authority provides the ability for pharmacists to practice at a high level, establishing pharmacy services requires some type of financial benefit to offset the salary of the pharmacist (through reimbursement in fee-for-service models or improved clinical outcomes in outcome-driven payment models). Without recognizing pharmacists as care providers, many healthcare institutions may struggle to recognize and support pharmacist roles, opting instead to utilize physicians, nurse practitioners, or physician assistants to meet patient needs easily addressed by pharmacists. Achievement of provider status in the United States is recognized by many pharmacy leaders as a high priority for the profession given its significant impact in supporting advanced pharmacist roles. In most settings, there is a shift away from pharmacist involvement in traditional compounding, preparation, and dispensing roles toward practicing as clinical pharmacists in patient care roles, usually as part of the healthcare team. The primary difference between one country and another is the status of this transition. Some countries are well along the pathway and have a significant portion of pharmacist time spent in a clinical role providing patient care, while others might be far more restrictive, just beginning this transition. There is also significant supporting evidence of the value that pharmacists bring as clinical pharmacists in these new roles, improving patient outcomes, safety, and lowering cost. In these cases, the pharmacist is responsible for and has the authority to select and order the initial dosage of medication, order necessary laboratory tests associated with the medication, and then to adjust the dosage and frequency of the medication based on the laboratory results. Examples of medications where this commonly occurs are vancomycin, aminoglycoside antibiotics, and other medications that require dosage adjustment based on the renal status of the patient.
Maintenance of fluid and electrolyte balance Fluid therapy during first 24 hour is of utmost importance arthritis diet plan 100 mg celebrex order mastercard. Optimum and rapid restoration of intravascular volume holds the key to rapid recovery. If the reaction has been caused by drugs with longer half-lives, the pathological processes may continue for a longer duration [19]. If administration of a class of drug is absolutely essential for the health of the patient, then the culprit medication should be substituted with a structurally unrelated molecule. The patient and the caregivers should then be asked history of the following: Onset, duration, and progression of the disease process. A detailed history of drug intake must be elicited (including ayurvedic/homeopathic/indigenous medicines or health supplements) prior to the onset of the eruptions, and efforts should be made to identify the likely offending drug. A thorough general, systemic, and cutaneous examination should be done including the following: Level of consciousness. Colloids are not preferred during the first 24 hours because of a risk of capillary leak [2]. Calculation of replacement fluid volume after 24 hours Maintenance fluid is titrated so as to maintain ideal urine output of 1 mL/kg/h (approximately 1500 mL/day) [27,29]. Monitoring Frequent monitoring of vital signs is essential to detect the first signs of a worsening systemic condition. Clinical Pulse rate (1/21 hour initially and later 2 hourly) Blood pressure (1/21 hour initially and later 2 hourly) Respiratory rate (1/21 hour initially and later 2 hourly) Anorectal temperature recording (perirectal thermometer must be used) Maintenance of fluid intake and urinary output chart Signs of sepsis [24] Sudden hypothermia with tachycardia and hypotension Fever or shivering after the fourth day in a euthermic patient Diminishing level of consciousness Change in mental status Falling urinary output Deterioration of respiratory status Loss of diabetic control Failure of gastric emptying Malena and hematemesis Any sudden change in the condition Note: Systemic steroids may mask the signs of sepsis. Periodicity of investigations: Complete blood count, daily Blood glucose, 12 hourly Serum electrolytes, 6 hourly Serum creatinine, daily Arterial blood gas analysis, 12 hourly Specific cultures, as mentioned earlier If facilities are available, septicemia and disseminated intravascular coagulation can be monitored Treatment of acute skin failure 15 by specialized tests such as coagulation assays, D-dimer assay, and fibrin degradation products. Nutritional support Aggressive nutritional support must be initiated early in order to Avoid metabolic disturbances Correct protein loss Promote healing Compensate the hypercatabolic state If oral intake is poor, nasogastric feeding is a preferred way of giving adequate nutrition [24]. If the residual gastric aspirate is more than 50 mL, feeding scheduled at that time should be withheld [8]. Topical antiseptics and dressings Burn-cage must be used since it gives protection from houseflies and dust and permits the patient to stay without tight dressings. However, some people feel that it increases (a) (b) evaporative loss and should be used only after stabilization of the patient [34]. Non infected detached epidermis and roof of deflated bullae serve as a biological dressing and hence should be retained. Biological dressings: Sterile banana leaves, potato peels, and amnion can be used. Collagen-based skin substitutes can also be used; however, they are expensive with limited availability. The secondary dressing needs to be changed due to soakage (generally in 23 days). Newer modalities include cadaveric allografts, cultured human allogeneic or autologous epidermal sheets, and human newborn fibroblasts cultured on a nylon mesh of Biobrane [36]. Mucocutaneous care Regular cleaning of mucous membranes prevents secondary infection and synechiae formation. Eye care For lid hygiene, regular normal saline wipes should be used to clean the eyelids while eyes are closed, from medial to lateral in a single stroke. With a single drop, the onset of anesthesia begins within 30 seconds and persists for 15 minutes or longer. Care of the oral cavity Conscious patients For cleaning, use a pediatric toothbrush and fluorinated toothpaste twice daily. Care of genitalia the genitalia, especially in case of females who have erosions on the opposing surfaces should be examined regularly. Apply white soft paraffin ointment twice daily to prevent the formation of synechiae and late sequelae such as scarring and fibrosis. Respiratory care Lung involvement may be complicated by pulmonary edema due to overzealous fluid replacement. Pooling of saliva and secretions may predispose to aspiration and therefore needs to be cleared frequently. Antibiotics that are commonly used are as follows [24]: Antistaphylococcal activity: Amoxicillin + clavulanic acid/tetracyclines/vancomycin/ clindamycin/teicoplanin/linezolid Gram-negative activity: Amikacin/piperacillin + tazobactam/cefoperazone + sulbactam/ imipenem) Anaerobic activity: Metronidazole/tinidazole Doses of different antibiotics that can be used are given in Table 2. Anticoagulation Deep vein thrombosis is a known complication in bedridden, old, debilitated, or obese patients. Photoprotection Should be advised for a few months to prevent chances of cutaneous pigmentary changes. Prevention of trophic/decubitus ulcers Examine the trophic ulcer prone sites-sacrum, ischial tuberosities, greater trochanters, and heels. Physiotherapy Physiotherapy is important to prevent deep venous thrombosis, help loosening of secretions in the respiratory tract, prevention of skeletal muscle weakness, and to facilitate early mobilization. Immediate stoppage of the offending drug/agent and treatment of the underlying condition are the keys for survival. Irrational, unwanted, and empirical use of drugs may further complicate the condition. Adequate hydration along with double-barrier nursing in a warm environment is the cornerstone of supportive management. Biological dressings that may be available in the future will reduce the use of antibiotics and reduce infections. A dedicated team of nursing staff, dermatologists, and cross consultation with other specialities are cornerstones for managing the acute failure of skin. Circulating vascular permeability factor/vascular endothelial growth factor in erythroderma. Toxic epidermal necrolysis and Stevens-Johnson syndrome: Does early withdrawal of causative drugs decrease the risk of death Committee for the development of guidelines for the prevention of vascular catheter associated infection; Indian society of critical care medicine.
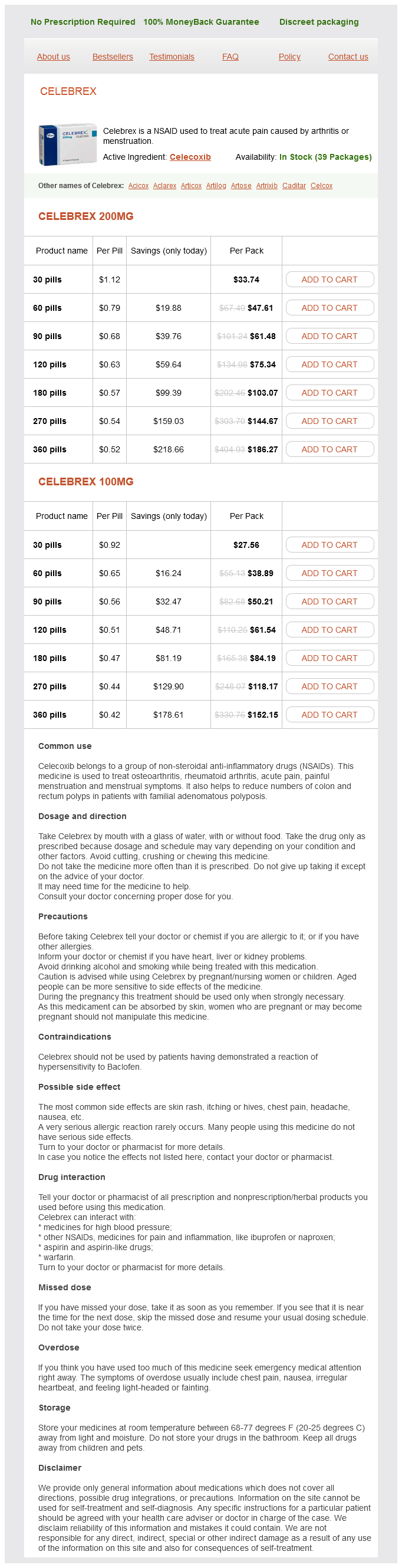
Celebrex Dosage and Price
Celebrex 200mg
- 30 pills - $33.74
- 60 pills - $47.61
- 90 pills - $61.48
- 120 pills - $75.34
- 180 pills - $103.07
- 270 pills - $144.67
- 360 pills - $186.27
Celebrex 100mg
- 30 pills - $27.56
- 60 pills - $38.89
- 90 pills - $50.21
- 120 pills - $61.54
- 180 pills - $84.19
- 270 pills - $118.17
- 360 pills - $152.15
Uterine serous carcinoma and endometrial intraepithelial carcinoma arising in endometrial polyps: Report of 5 cases arthritis back chiropractic order celebrex online pills, including 2 associated with tamoxifen therapy. Stromal p16 expression differentiates endometrial polyp from endometrial hyperplasia. Uterine adenomyoma: A clinicopathologic review of 26 cases and a review of the literature. Uterine adenomyomas excluding atypical polypoid adenomyomas and adenomyomas of endocervical type: A clinicopathologic study of 30 cases of an underemphasized lesion that may cause diagnostic problems with brief consideration of adenomyomas of other female genital tract sites. Adenomyomatous polyp of the endometrium with prominent epithelioid smooth muscle differentiation: Report of two cases of a hitherto undescribed lesion. Atypical polypoid adenomyoma of the uterus: An immunohistochemical and molecular study of 21 cases. Takahashi H, Yoshida T, Matsumoto T, Kameda Y, Takano Y, Tazo Y, Inoue H, Saegusa M. Immunohistochemical characteristics of atypical polypoid adenomyoma with special reference to h-caldesmon. A comparative morphologic and immunohistochemical analysis of 33 highly cellular leiomyomas and six endometrial stromal nodules, two frequently confused tumors. Endometrial stromal nodules and endometrial stromal tumors with limited infiltration: A clinicopathologic study of 50 cases. An immunohistochemical analysis of endometrial stromal and smooth muscle tumors of the uterus: A study of 54 cases emphasizing the importance of using a panel because of overlap in immunoreactivity for individual antibodies. Mullerian adenosarcoma: A clinicopathologic and immunohistochemical study of 55 cases challenging the existence of adenofibroma. Adenofibroma and adenosarcoma of the uterus: A clinicopathologic study of 35 cases. Müllerian adenofibroma of the uterus with invasion of myometrium and pelvic veins. Adenomyomas of the uterine cervix: Report of a cohort including endocervical and novel variants. Florid reactive lymphoid hyperplasia of the lower female genital tract (lymphoma-like lesion): A benign condition that frequently harbors clonal immunoglobulin heavy chain gene rearrangements. Plexiform tumorlet: A clinical and pathologic study of 15 cases with ultrastructural observations. Uterine and extrauterine plexiform tumourlets are sex-cord-like tumours with myoid features. Plexiform tumorlet of the uterus: Immunohistological evidence for a smooth muscle origin. Diverse phenotypic profile of uterine tumors resembling ovarian sex cord tumors: An immunohistochemical study of 12 cases. Endometrial metaplasias and reactive changes: A spectrum of altered differentiation. Endometrial epithelial metaplasias: Proliferations frequently misdiagnosed as adenocarcinoma. Dysplastic Ichthyosis uteri-like changes of the entire endometrium associated with a squamous cell carcinoma of the uterine cervix. Eosinophilic cell change of the endometrium: A possible relationship to mucinous differentiation. Oncocytic metaplasia and carcinoma of the endometrium: An immunohistochemical and ultrastructural study. Mucinous endometrial epithelial proliferations: A morphologic spectrum of changes with diverse clinical significance. Atypical mucinous glandular proliferations in endometrial samplings: Follow-up and other clinicopathological findings in 41 cases. Endometrial histopathology in 700 patients treated with tamoxifen for breast cancer. Endometrial intestinal metaplasia: A report of two cases, including one associated with cervical intestinal and pyloric metaplasia. Reappraisal of synchronous and multifocal mucinous lesions of the female genital tract: A close association with gastric metaplasia. Papillary syncytial metaplasia associated with endometrial breakdown exhibits an immunophenotype that overlaps with uterine serous carcinoma. Simple and complex hyperplastic papillary proliferations of the endometrium: A clinicopathologic study of nine cases of apparently localized papillary lesions with fibrovascular stromal cores and epithelial metaplasia. Papillary proliferation of the endometrium: A clinicopathologic study of 59 cases of simple and complex papillae without cytologic atypia. Endometrial synovial-like metaplasia associated with levonorgestrel-releasing intrauterine system. Heterotopic adipose and glial tissue in the endometrium with staining for glial fibrillary acidic protein. Fetal glial allograft in the endometrium: Case report of a recurrent pseudo-tumor. Endometrial premalignant lesions, which are commonly referred as precursors or precancers of the endometrium, are less illustrated compared to those malignant counterparts. Putative precursors of endometrial clear-cell carcinoma have been briefly described in the past. There is no precursor of endometrial mucinous, poorly differentiated or undifferentiated or de-differentiated carcinomas described. In this article, we will focus on the precursors of endometrioid and serous cancers. Unfortunately, this classification system has been dropped due to its poor reproducibility even among gynecological pathologists. Simply put, the endometrial glandularto-stroma ratio is over 1 in a defined endometrial tissue sample.
© 2025 Adrive Pharma, All Rights Reserved..