General Information about Cefixime
One of the major benefits of cefixime is its capacity to be taken orally. This signifies that sufferers can take the treatment at home, without the necessity for hospital visits or intravenous treatment. This makes it a extra handy possibility for many who cannot or don't wish to be hospitalized. Cefixime is out there within the form of tablets, capsules, and oral suspension, making it straightforward for individuals of all ages to use.
Like some other treatment, cefixime additionally has some unwanted effects. The commonest ones embrace diarrhea, nausea, belly pain, and allergic reactions corresponding to skin rash and itching. In uncommon instances, it can additionally cause extreme side effects like liver and kidney issues. It is important to follow the prescribed dosage and consult a well being care provider if any unwanted facet effects are skilled.
Cefixime is a extensively used antibiotic belonging to the cephalosporin group of medication. It is commonly prescribed by doctors to deal with quite a lot of bacterial infections such as respiratory tract infections, urinary tract infections, and ear infections. This drug has proven to be effective in fighting in opposition to a quantity of forms of bacteria and has gained recognition because of its ease of use and fewer unwanted effects.
As with any antibiotic, it is essential to use cefixime judiciously and solely when prescribed by a physician. Overuse or misuse of antibiotics can result in the development of drug-resistant bacteria, making the medication much less efficient in the lengthy term. It is also necessary to finish the total course of treatment, even when the symptoms improve, to make sure that the an infection is completely eradicated.
In conclusion, cefixime is a broadly used and efficient antibiotic in the therapy of varied bacterial infections. Its oral type of administration, broad spectrum of motion, and fewer unwanted aspect effects make it a preferred choice for medical doctors and patients alike. It is essential to make use of this medication responsibly and under medical supervision to make sure its effectiveness and keep away from any potential unwanted effects.
Cefixime is generally thought-about safe to be used in pregnant and breastfeeding ladies. However, it is all the time advisable to consult a well being care provider earlier than taking any medication during being pregnant or whereas breastfeeding.
Cefixime works by interfering with the formation of the bacterial cell wall, thus stopping the expansion and multiplication of bacteria. It belongs to the third generation cephalosporin class of antibiotics, which makes it more potent and effective towards a broader spectrum of bacteria than its previous generations. This makes it a most popular choice for many medical doctors when it comes to treating bacterial infections.
Cefixime is primarily used to deal with infections attributable to bacteria corresponding to Streptococcus, Streptococcus pneumoniae, Haemophilus influenzae, E. coli, and Klebsiella pneumoniae. It is very efficient in treating infections in the respiratory tract, such as pneumonia, bronchitis, and sinusitis. It can also be generally used to treat urinary tract infections, corresponding to cystitis and pyelonephritis. In some instances, it can additionally be used to treat ear infections, sexually transmitted infections, and different bacterial infections in the physique.
The nucleus solitarius virus 000 purchase cheap cefixime online, located in the cardiovascular center of the medulla, receives impulses from these stretch receptors through afferents of the glossopharyngeal and vagus nerves. The cardiovascular center in the medulla consists of two functionally different areas; the area responsible for increasing blood pressure is laterally and rostrally located, whereas the area responsible for lowering arterial blood pressure is centrally and caudally located. The latter area also integrates impulses from the hypothalamus and the limbic system. Typically, stretch receptors are activated if systemic blood pressure is greater than 170 mm Hg. The response of the depressor system includes decreased sympathetic activity, leading to a decrease in cardiac contractility, heart rate, and vascular tone. In addition, activation of the parasympathetic system further decreases the heart rate and myocardial contractility. The baroreceptor reflex plays an important beneficial role during acute blood loss and shock. However, the reflex arch loses its functional capacity when arterial blood pressure is less than 50 mm Hg. Chemoreceptor Reflex Chemosensitive cells are located in the carotid bodies and the aortic body. At an arterial partial O2 pressure (PaO2) of less than 50 mm Hg or in conditions of acidosis, the chemoreceptors send their impulses along the sinus nerve of Hering (a branch of the glossopharyngeal nerve) and the tenth cranial nerve to the chemosensitive area of the medulla. This area responds by stimulating the respiratory centers and thereby increasing ventilatory drive. In addition, activation of the parasympathetic system ensues and leads to a reduction in heart rate and myocardial contractility. Bainbridge Reflex the Bainbridge reflex85-87 is elicited by stretch receptors located in the right atrial wall and the cavoatrial junction. An increase in right-sided filling pressure sends vagal 14 · Cardiac Physiology 401 afferent signals to the cardiovascular center in the medulla. These afferent signals inhibit parasympathetic activity, thereby increasing the heart rate. The changes in heart rate are dependent on the underlying heart rate before stimulation. Administration of an antimuscarinic drug such as glycopyrrolate or atropine reduces the incidence of bradycardia during eye surgery. Johanna Schwarzenberger and Radhika Dinavahi for their contribution to this chapter in the prior edition of this work. Bezold-Jarisch Reflex the Bezold-Jarisch reflex responds to noxious ventricular stimuli sensed by chemoreceptors and mechanoreceptors within the left ventricular wall by inducing the triad of hypotension, bradycardia, and coronary artery dilatation. Because it invokes bradycardia, the Bezold-Jarisch reflex is thought of as a cardioprotective reflex. This reflex has been implicated in the physiologic response to a range of cardiovascular conditions such as myocardial ischemia or infarction, thrombolysis, or revascularization and syncope. Thus, the Bezold-Jarisch reflex may be less pronounced in patients with cardiac hypertrophy or atrial fibrillation. This decrease will be sensed by baroreceptors and will reflexively result in an increase in heart rate and myocardial contractility through sympathetic stimulation. When the glottis opens, venous return increases and causes the heart to respond by vigorous contraction and an increase in blood pressure. This increase in arterial blood pressure will, in turn, be sensed by baroreceptors, thereby stimulating the parasympathetic efferent pathways to the heart. Cushing Reflex the Cushing reflex is a result of cerebral ischemia caused by increased intracranial pressure. Cerebral ischemia at the medullary vasomotor center induces initial activation of the sympathetic nervous system. Such activation will lead to an increase in heart rate, arterial blood pressure, and myocardial contractility in an effort to improve cerebral perfusion. As a result of the high vascular tone, reflex bradycardia mediated by baroreceptors will ensue. Oculocardiac Reflex the oculocardiac reflex is provoked by pressure applied to the globe of the eye or traction on the surrounding structures. Once activated, stretch receptors will send afferent signals through the short- and long-ciliary nerves. The ciliary nerves will merge with the ophthalmic division of the trigeminal nerve at the ciliary ganglion. The trigeminal nerve will carry these impulses to the gasserian ganglion, thereby resulting in increased parasympathetic tone and subsequent bradycardia. William Harvey and the circulation of the blood: the birth of a scientific revolution and modern physiology. Mechanisms underlying the increase in force and Ca2+ transient that follow stretch of cardiac muscle. Desmin cytoskeleton: a potential regulator of muscle mitochondrial behavior and function. Cardiac alpha(1)-adrenoceptors that regulate contractile function: subtypes and subcellular signal transduction mechanisms. Minireview: natriuretic peptides during development of the fetal heart and circulation. Sex dimorphism in cardiac pathophysiology: experimental findings, hormonal mechanisms, and molecular mechanisms. Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Sinusoidal neck suction for evaluation of baroreflex sensitivity during desflurane and sevoflurane anesthesia.
The most prevailing test to evaluate gastric motility is the gastric emptying study will antibiotics for uti help kidney infection cefixime 100 mg buy without prescription. The patient fasts for at least 4 hours prior to the study then consumes a meal with a tightly bound radiotracer, commonly egg albumin. Continuous or frequent imaging occurs for the next 60 to 120 minutes and the measurement of time for 50% of the ingested meal to empty is determined. It is important to note that while 15 · Gastrointestinal Physiology and Pathophysiology 407 gastric emptying scintigraphy has long been the standard study, it is affected by multiple factors including meal composition and data acquisition parameters. Small intestinal motility mixes the contents of the stomach with digestive enzymes, further reducing particle size and increasing solubility. However, the major function of the small intestine is to circulate the contents and expose them to the mucosal wall in order to maximize absorption of water, nutrients, and vitamins before entering the large intestine. The circular and longitudinal muscle layers work in a coordinated fashion to achieve segmentation. Segmentation occurs when two nearby areas contract and thereby isolate a segment of intestine. Then a contraction occurs in the middle of that isolated segment, further dividing it. Contractions in the middle of those segments continue to occur and the process ensues. Segmentation allows the contents to remain in the intestine long enough for the essential substances to be absorbed into the circulation. It is controlled mainly by the enteric nervous system with modulation of motility by the extrinsic nervous system. When considering small bowel dysmotility it is helpful to distinguish etiologies based on reversible and nonreversible causes. For reversible causes, mechanical obstruction should be the first to come to mind. In this case, there is a physical obstruction the muscles of the intestine cannot overcome. Although the large intestine is rich with bacteria, the small intestine usually has fewer than 100,000 organisms per milliliter. Disrupting this condition with bacterial overgrowth leads to alterations in absorptive function leading to diarrhea. Other reversible causes include ileus, electrolyte abnormalities, and critical illness. In structural causes there may be abnormalities with the intestinal smooth muscle, in which it cannot produce proper contractions. Short bowel syndrome can be considered a structural etiology in that a large portion of the small intestinal structure is simply not present. In patients who have had a section of their small bowel resected, the remaining portion may not provide sufficient functional compensation, resulting in diarrhea, malnutrition, and weight loss. Neuropathic etiologies can produce a pseudo-obstruction in which the intrinsic and extrinsic nervous systems are altered in such a way that the intestines can only produce weak or uncoordinated contractions. Regardless of etiology, small intestinal dysmotility adversely affects nutrient absorption leading to malnutrition. The most common test used to evaluate small intestine motility is small bowel manometry. This test is useful in patients with unexplained nausea, vomiting, abdominal pain, and manifested signs of obstruction without a clear obstructive cause. Similar to esophageal manometry, this test uses a small catheter with pressure sensors to evaluate the contractions of the intestine. The study evaluates contractions during three periods: fasting, during a meal, and postprandial. Normally the recording time is four hours for fasting, followed by ingestion of a meal, and two hours postprandial. In neuropathic results, the contraction amplitude is adequate but either the contractions are uncoordinated (enteric neuropathy) or there is an inappropriate postprandial response, meaning postprandial antral hypomotility is present (extrinsic neuropathy). This manometry test is reported to result in a change of diagnosis in 8% to 15% of patients with unexplained nausea, vomiting, and abdominal pain. Distention of the ileum will relax the ileocecal valve to allow intestinal contents to enter the colon and subsequent cecal distention will contract it. While there are still mixing and propulsive movements by the circular and longitudinal muscles, respectively, the colon also exhibits giant migrating complexes. The giant migrating complexes serve to produce mass movements across the large intestine. In the healthy state, these complexes occur approximately 6 to 10 times within 24 hours with mean amplitude of 115 mm Hg at a distance of about 1 cm/s for approximately 20 seconds each. The giant migrating complexes that originate in the sigmoid colon will produce the urge to defecate. Colonic dysmotility manifests with two primary symptoms: altered bowel habits and intermittent abdominal cramping. In addition, there is a depression of overall contractile activity in the colon leading to colonic distention and the sensation of pain. This phenomenon is exacerbated by stress in which there is significant motor dysfunction and visceral hypersensitivity as well as an increase in plasma norepinephrine stimulating the sympathetic nervous system.
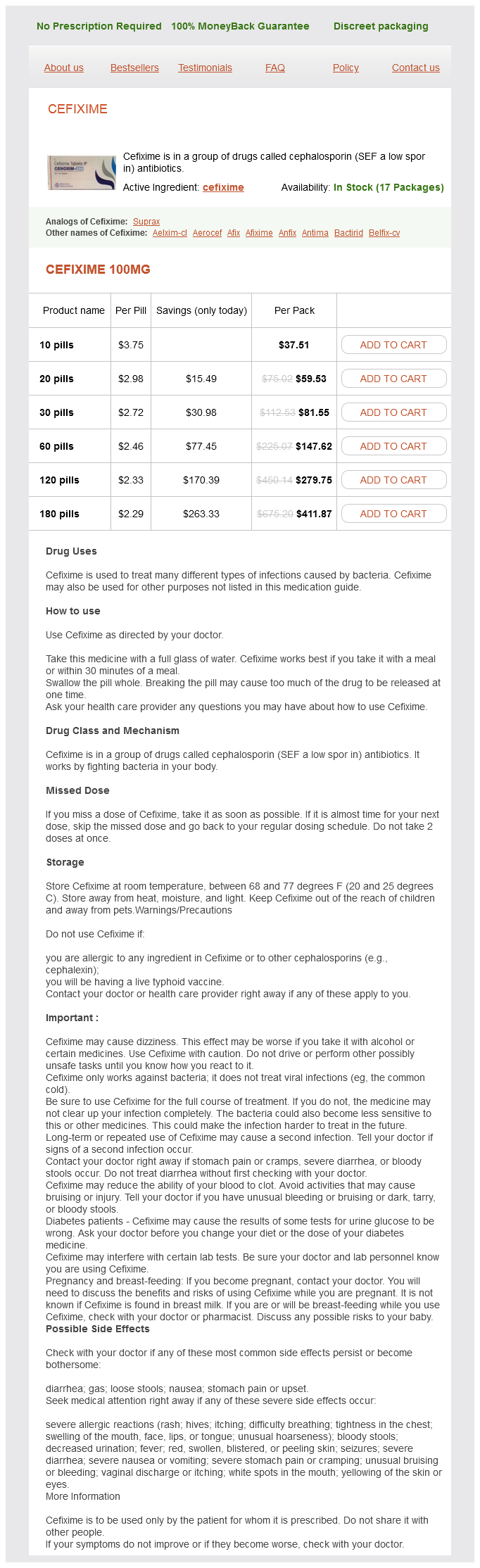
Cefixime Dosage and Price
Cefixime 100mg
- 10 pills - $37.51
- 20 pills - $59.53
- 30 pills - $81.55
- 60 pills - $147.62
- 120 pills - $279.75
- 180 pills - $411.87
Hypoxic pulmonary vasoconstriction does not contribute to pulmonary blood flow heterogeneity in normoxia in normal supine humans antibiotics for uti during pregnancy cheap cefixime 100 mg buy. Role of airway nitric oxide on the regulation of pulmonary circulation by carbon dioxide. Hypoxia induces the release of a pulmonary-selective, Ca(2+)-sensitising, vasoconstrictor from the perfused rat lung. Ca(2+) release from ryanodine-sensitive store contributes to mechanism of hypoxic vasoconstriction in rat lungs. Mitochondria-dependent regulation of Kv currents in rat pulmonary artery smooth muscle cells. Hypoxic pulmonary vasoconstriction requires connexin 40-mediated endothelial signal conduction. General anesthetics and vascular smooth muscle: direct actions of general anesthetics on cellular mechanisms regulating vascular tone. Endothelium-dependent pulmonary vasodilation is selectively attenuated during isoflurane anesthesia. Halothane and enflurane attenuate pulmonary vasodilation mediated by adenosine triphosphate-sensitive potassium channels compared to the conscious state. Pulmonary vasodilator response to adenosine triphosphate-sensitive potassium channel activation is attenuated during desflurane but preserved during sevoflurane anesthesia compared with the conscious state. Isoflurane and the pulmonary vascular pressure-flow relation at baseline and during sympathetic alphaand beta-adrenoreceptor activation in chronically instrumented dogs. Effects of halothane and enflurane anesthesia on sympathetic beta-adrenoreceptor-mediated pulmonary vasodilation in chronically instrumented dogs. Volatile anesthetics regulate pulmonary vascular tension through different potassium channel subtypes in isolated rabbit lungs. Attenuated hypoxic pulmonary vasoconstriction during isoflurane anesthesia is abolished by cyclooxygenase inhibition in chronically instrumented dogs. Endothelium-derived relaxing factor is not responsible for inhibition of hypoxic pulmonary vasoconstriction by inhalational anesthetics. Isoflurane anesthesia attenuates endothelium-dependent pulmonary vasorelaxation by inhibiting the synergistic interaction between nitric oxide and prostacyclin. Role of potassium channels in isoflurane- and sevoflurane-induced attenuation of hypoxic pulmonary vasoconstriction in isolated perfused rabbit lungs. Preservation of hypoxic pulmonary vasoconstriction during sevoflurane and desflurane anesthesia compared to the conscious state in chronically instrumented dogs. The effects of xenon or nitrous oxide supplementation on systemic oxygenation and pulmonary perfusion during one-lung ventilation in pigs. Anesthetic effects on synaptic transmission and gain control in respiratory control. The variable effect of low-dose volatile anaesthetics on the acute ventilatory response to hypoxia in humans: a quantitative review. Effect of low dose inhaled anaesthetic agents on the ventilatory response to carbon dioxide in humans: a quantitative review. Reconfiguration of the pontomedullary respiratory network: a computational modeling study with coordinated in vivo experiments. An interdependent model of central/peripheral chemoreception: evidence and implications for ventilatory control. Termination of inspiration by phase-dependent respiratory vagal feedback in awake normal humans. Comparison of the response of diaphragm and upper airway dilating muscle activity in sleeping cats. Lung volume and collapsibility of the passive pharynx in patients with sleep-disordered breathing. Lung perfusion, shunt fraction, and oxygenation during one-lung ventilation in pigs: the effects of desflurane, isoflurane, and propofol. The effects of increasing concentrations of desflurane on systemic oxygenation during one-lung ventilation in pigs. The effects of increasing concentrations of isoflurane and desflurane on pulmonary perfusion and systemic oxygenation during one-lung ventilation in pigs. Isoflurane and sevoflurane anesthesia in pigs with a preexistent gas exchange defect. Inhalation anesthesia increases V/Q regional heterogeneity during spontaneous breathing in healthy subjects. Spontaneous breathing during general anesthesia prevents the ventral redistribution of ventilation as detected by electrical impedance tomography: a randomized trial. Effects of spontaneous breathing, mechanical ventilation and positive endexpiratory pressure. N omega-nitro-L-arginine and pulmonary vascular pressure-flow relationship in conscious dogs. Arterial oxygenation and shunt fraction during one-lung ventilation: a comparison of isoflurane and sevoflurane. A comparison of the effects of propofol-alfentanil versus isoflurane anesthesia on arterial oxygenation during one-lung ventilation. Effects of sevoflurane and propofol on pulmonary shunt fraction during one-lung ventilation for thoracic surgery. Effects of propofol vs sevoflurane on arterial oxygenation during one-lung ventilation. Comparison of the effects of propofol and isoflurane anaesthesia on right ventricular function and shunt fraction during thoracic surgery. The effects of propofol, isoflurane, and sevoflurane on oxygenation and shunt fraction during one-lung ventilation.
© 2025 Adrive Pharma, All Rights Reserved..