General Information about Calcitriol
Vitamin D is crucial for the traditional functioning of the human body. It is crucial for the absorption of calcium and phosphorus from the food regimen, which are essential for maintaining healthy bones. Vitamin D is produced within the body when the skin is exposed to daylight, and it can be obtained from dietary sources similar to dairy merchandise, fatty fish, and egg yolks.
Calcitriol, also known by its model name Rocaltrol, is a drugs that belongs to the class of medication called vitamin D analogues. It is used to deal with circumstances attributable to an absence of vitamin D, corresponding to certain bone issues like osteoporosis and osteomalacia. Calcitriol works by increasing the absorption of calcium from the intestines and selling its deposition into the bones, thus serving to keep healthy bone density and energy.
One of the principle uses of Calcitriol is to treat osteoporosis, a situation characterised by weak and brittle bones. This situation is more prevalent in older adults and postmenopausal women due to hormonal modifications that happen throughout menopause. It can also happen in people with persistent kidney disease, liver disease, and those on long-term steroid medicines. Calcitriol helps stop the event of osteoporosis by increasing the absorption of calcium from the diet, which is significant for maintaining strong bones.
Apart from its function in bone well being, Calcitriol can be used to deal with different medical circumstances similar to chronic kidney disease, where it helps scale back the build-up of calcium within the blood and keep normal ranges of phosphate. It can also be prescribed for individuals with hypoparathyroidism, a condition where the parathyroid gland does not produce sufficient parathyroid hormone, which might lead to low levels of calcium within the blood. Calcitriol promotes the absorption of calcium from the food regimen and helps maintain normal levels within the blood.
Calcitriol can additionally be used within the therapy of osteomalacia, a situation that causes gentle and weak bones because of a lack of vitamin D. This condition is more frequent in adults who've a diet low in vitamin D or have reduced solar exposure as a end result of living in areas with restricted daylight. Calcitriol restores the levels of vitamin D within the physique, promoting the absorption of calcium and phosphorus, and reversing the signs of osteomalacia.
However, there are certain groups of people that may be at threat of vitamin D deficiency, such as those who have restricted solar exposure, those with dark skin, and individuals with sure medical circumstances that can interfere with the absorption of vitamin D. In such circumstances, supplementation with Calcitriol may be needed to forestall deficiencies and preserve proper bone well being.
Calcitriol is usually taken orally in the form of capsules or liquid, and the dosage is decided by a health care provider based on an individual's medical situation and response to therapy. It is essential to comply with the prescribed dosage and not exceed it, as extreme ranges of vitamin D within the body can lead to toxicity. Common unwanted effects of Calcitriol include nausea, vomiting, and lack of urge for food. Serious unwanted effects corresponding to high ranges of calcium within the blood, irregular heartbeat, or kidney problems are rare but should be reported to a healthcare skilled instantly.
In conclusion, Calcitriol, or Rocaltrol, is a vital medicine for maintaining healthy bones and treating circumstances caused by vitamin D deficiency. It is an effective therapy for osteoporosis, osteomalacia, and other medical conditions that may affect bone health. However, it is essential to take it as prescribed and to observe the levels of calcium within the blood to forestall any problems. Consult a health care provider for extra info on Calcitriol and its potential benefits for your individual health needs.
Lesions of mucous membrane (cicatricial) pemphigoid are usually confined to the oral mucosa or conjunctivae and occur in patients older than 50 years medicine 44-527 buy calcitriol 0.25 mcg. They begin as vesicles that quickly rupture, leaving ulcers that are chronic but only moderately symptomatic. In this latter group, the lesions of mucosal lupus may be analogous to the skin lesions of chronic discoid lupus. They take the form of reticular hyperkeratotic figures associated with erythema, often resembling lichen planus, but unlike lichen planus are usually solitary or bilaterally asymmetrical. They begin as macules with a blue or purple color, at which time they must be distinguished from purpura. Similar lesions may be present at the border of an ill-fitting denture or may occur in clusters on the hard palate under an ill-fitting denture (palatal papillomatosis). Generalized or multifocal enlargement of the gingiva (gingival hyperplasia) may be caused by chronic administration of phenytoin, cyclosporine, and many of the calcium-channel blocking drugs. It can also be associated with a hereditary defect or be caused by an infiltration of atypical white blood cells in some types of leukemia (particularly acute monocytic leukemia; Chapter 183) or by uncontrolled diabetes mellitus (Chapter 229). They are occasionally classified as epithelial neoplasms, but most do not continue to grow. Human papillomavirus types 2, 6, 11, 13, 32, and 57 have been identified in these wartlike Pigmentations Brown or gray-black macules on the oral mucosa are relatively common and range from benign to highly malignant. They may be caused by localized increase in melanin production, proliferation of melanin-producing cells, or deposition of local or systemically distributed pigmented substances Table 425-4). Mucosal pigmentation may occur after long-term administration of hydroxychloroquine, minocycline, ketoconazole, methyldopa, or cyclophosphamide. Malignant melanomas can occur at any oral mucosal site, but about 85% develop on the hard palatal mucosa or gingiva, or both. Most salivary gland tumors in the parotid gland are benign, in contrast to the sublingual gland, where more than 90% are malignant. Benign tumors are generally slowly growing, not fixed to the skin, and do not show ulceration. Malignancies generally grow more quickly, are often fixed to the skin or adjacent normal structures, and tend to show ulceration. Adenoid cystic carcinoma has a characteristic local infiltration by perineural spread. Detection of any salivary gland mass lesions should be followed by appropriate imaging, cytology, and biopsy. A large wartlike lesion on the oral mucosa should raise suspicion of verrucous carcinoma. MucousRetentionLesions(Mucoceles) Mucoceles are small, chronic, or recurring vesicles or bullae that occur commonly on the inside of the cheeks and lips, the posterior palate, and the mouth floor. They are caused by injury to one of the many submucosal minor salivary glands, resulting in extravasation of mucus, which causes granulomatous inflammation or blockage of the excretory duct, leading to cyst formation. Both types of lesions require conservative surgical excision because simple incision and drainage are usually followed by recurrence. Any exudate should be cultured, and initial treatment should be with an oral penicillinase-resistant antibiotic, such as cloxacillin or dicloxacillin, 500 mg, every 6 hours. More than 20 types of benign or malignant neoplasms appear as firm and nontender unilateral or bilateral enlargement of a major gland or as a firm submucosal nodule on the palate or the labial or buccal mucosa Table 4256). Uncommonly, unilateral major gland enlargement may be reactive-for example, chronic sialadenitis from duct obstruction or inadequately treated bacterial sialadenitis. Salivary gland tumors are relatively uncommon and usually present as a swelling in one of the major paired salivary glands or in one of the minor glands of the mouth. The most common benign salivary gland the best-known cause of bilateral salivary gland enlargement is infection by the mumps virus (Chapter 369) in children. However, the prevalence of mumps decreased in the United States by more than 98% after the introduction of an effective vaccine in 1967, and now there are only a few hundred to a few thousand cases per year. Uncommonly, a less acute, mumps-like illness may occur in adults in association with cytomegalovirus (Chapter 376), influenza (Chapter 364), or Coxsackie A (Chapter 379) virus infection. Histologically, the tumors begin as a benign lymphoepithelial lesion (myoepithelial sialadenitis), but after years of chronicity, some transform into an extranodal marginal zone lymphoma (Chapter 185). Several chronic granulomatous diseases, such as sarcoidosis (Chapter 95), tuberculosis (Chapter 324), and leprosy (Chapter 326), can cause bilateral enlargement and decreased function of salivary glands. Parotid gland enlargement usually represents a solid or cystic lymphoepithelial lesion (see Table 425-2). Recurrent parotitis of childhood includes episodes of unilateral or bilateral parotid enlargement. During flares of this illness, salivary secretion may be reduced, but usually without prominent secondary symptoms or signs. Parotid glands can develop bilateral, symmetrical enlargement that is soft and nontender to palpation and associated with normal salivary function (see Table 425-6). Diagnosis is established by this clinical presentation and the presence of one of the systemic diseases known to be associated with it: diabetes mellitus (Chapter 229), hyperlipoproteinemia (Chapter 206), hepatic cirrhosis (Chapter 153), anorexia or bulimia (Chapter 219), chronic pancreatitis (Chapter 144), acromegaly (Chapter 224), and gonadal hypofunction. It can also result from use of phenylbutazone or be a reaction to iodine-containing contrast media. Periodontal disease in its most prevalent form is associated with excessive build-up of plaque on teeth and roots. Most cases of periodontal disease begin with inflammation of the gingiva-termed gingivitis-that may progress to loss of the supporting bone around the roots of the teeth. Other subtypes of periodontal disease are recognized with differing risk factors and natural histories. The mainstay of treatment is the removal of subgingival calculus and biofilm deposits using mechanical methods (tooth brushing, flossing, scaling, and root planing). Despite ongoing concerns, there is no current evidence that periodontal disease is an independent risk factor for coronary artery disease.
The distribution of visual function across the retina takes a pattern of concentric zones increasing in sensitivity toward the center medicine nobel prize 2015 purchase 0.25 mcg calcitriol with amex, the fovea. The fovea consists of a "rod-free" central grouping of approximately 100,000 slender cones. The ganglion cells subserving these cones send their axons directly to the temporal aspect of the optic disc, where they form the papillomacular bundle. Axons originating from ganglion cells in the temporal retina curve above and below the papillomacular bundle and form dense arcuate bands. The arteries supplying the optic nerve and retina derive from branches of the ophthalmic artery. The central retinal artery approaches the eye along each optic nerve and pierces the inferior aspect of the dural sheath about 1 cm behind the globe to enter the center of the nerve. The artery emerges in the fundus at the center of the nerve head, from which it nourishes the inner two thirds of the retina by superior and inferior branches. Anastomotic branches derived from the choroidal and posterior ciliary arteries, the ciliary system, supply the choroid, optic nerve head, and outer retinal layers, including the photoreceptors. In about 10% of the population, the macula is supplied by a retinociliary artery, a branch of the ciliary system. Venous drainage from the retina and nerve head flows primarily through the central retinal vein, whose course of exit from the eye parallels that of entry of the artery. The nasal side of the left retina and the temporal side of the right see the left side of the world, and the upper half of each retina sees the lower half of the world. Behind the eyes, the optic nerves pass through the optic canal to form the optic chiasm. In the chiasm, nerves from the nasal half of each retina decussate and join the fibers from the temporal half of the contralateral retina. From the chiasm, the optic tracts pass around the cerebral peduncles to reach the lateral geniculate ganglia. The orientation of the visual field is rotated 90 degrees in the lateral geniculate such that images from the inferior visual field project to the medial half, whereas images from the superior visual field project to the lateral half. Atropine vs patching for treatment of moderate amblyopia: follow-up at 15 years of age of a randomized clinical trial. American Joint Committee on Cancer T category for eyelid sebaceous carcinoma correlates with nodal metastasis and survival. Prevalence, treatment, and outcomes of coexistent ocular surface squamous neoplasia and pterygium. Six-year incidence of endophthalmitis after cataract surgery: Swedish national study. Treatment of infantile capillary hemangioma of the eyelid with systemic propranolol. Diagnostic performance of magnetic resonance imaging and computed tomography for advanced retinoblastoma: a systematic review and meta-analysis. Answer: A At age 45 years, the amount of available accommodative reserve decreases to the point at which reading and other near tasks become difficult. Although cataracts can occur at age 45 years, the incidence is very low, and such early cataracts are usually unilateral. A serous detachment of the retina usually occurs in one eye and causes acquired asymmetrical vision. Scarring of the internal surface of the retina (epiretinal membrane formation) is also usually a unilateral abnormality. Neovascularization of the external surface of the retina (subretinal neovascularization) is also usually a unilateral acquired abnormality. A 35-year-old man developed mild focal upper eyelid pain and swelling associated with a tender mass. Answer: B Unilateral eyelid pain and swelling is the usual presentation of a chalazion (rupture of a meibomian gland). A stye, which is an abscess of a pilosebaceous unit, presents with extreme pain and the risk for anterior or posterior cellulites. Blockage of an eccrine duct (ductal cyst) is also painless and usually occurs in the conjunctiva. Proliferation of non-nodal lymphoid tissue (lymphoma) is also painless and usually found in the upper or lower fornix of the conjunctiva. A 43-year-old near-sighted man notes the sensation of flashing lights and an increased number of small floaters in the right eye. This afternoon during his annual physical examination, he notes loss of the inferior visual field of that eye. Schedule for next available eye examination Answer: D Recent onset of the sensation of floaters and flashing lights is the common presentation of retinal detachment. A 71-year-old man has noted halos around oncoming car headlights and double vision in only one eye. Increase of refractive index of the lens Answer: E Monocular diplopia (diplopia with one eye open) is a common presentation of a cataract, although corneal surface abnormalities may present similarly. The other conditions present with bilateral diplopia (diplopia disappears with closure of one eye). The notation in a drug insert states that the drug should not be used if the patient has glaucoma.
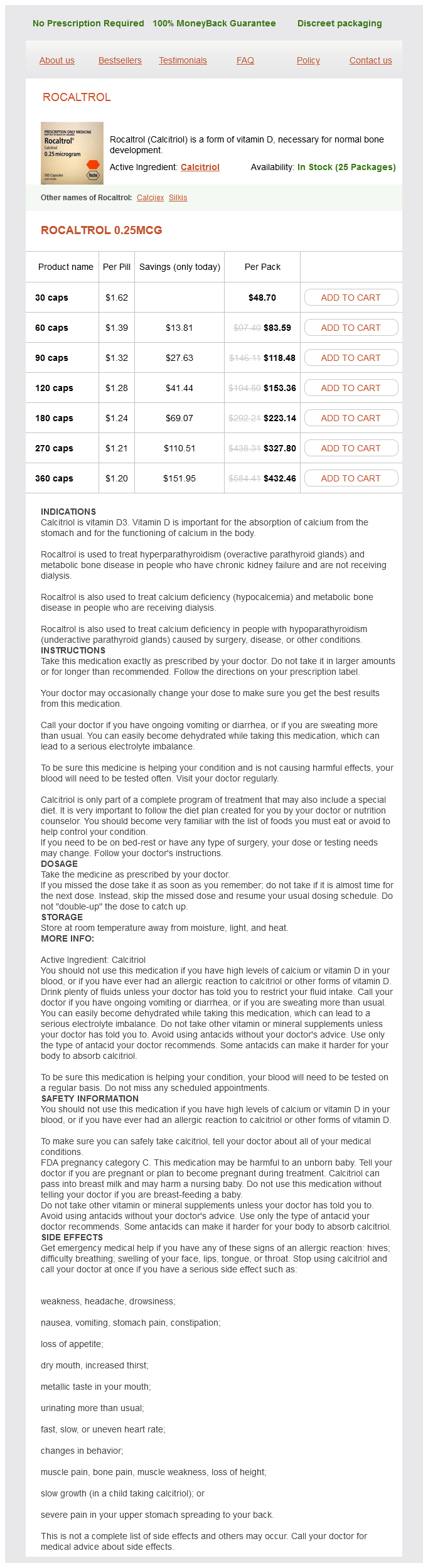
Calcitriol Dosage and Price
Rocaltrol 0.25mcg
- 30 caps - $48.70
- 60 caps - $83.59
- 90 caps - $118.48
- 120 caps - $153.36
- 180 caps - $223.14
- 270 caps - $327.80
- 360 caps - $432.46
In the extreme medicine online quality 0.25 mcg calcitriol, chemosensory disorders can lead to overwhelming stress, anorexia, and depression. Genes that encode chemoreceptor proteins belong to the G proteincoupled receptor superfamily, which accounts for up to 1% of mammalian genomes. Pathophysiology Disorders of taste and smell can be divided into local, systemic, and neurologic categories Table 427-1). A patient without other systemic disease or immunocompromise presents with otitis externa confined to the external auditory canal. The physician should order a computed tomographic scan with contrast of the temporal bone. Oral or systemic antibiotics are specifically not recommended unless the patient is immunocompromised or the infection is spreading to the pinna cartilage of the external ear outside of the external auditory canal. The patient should be admitted to the hospital for interventional embolization of the internal maxillary artery. The patient should be queried about aspirin use and be asked to take an "aspirin holiday. Answer: D Patients with epistaxis are often on antiplatelet drugs for a variety of reasons. On intake history, use of nonsteroidal anti-inflammatory drugs should be specifically sought because curtailing antiplatelet medication will often eliminate troublesome epistaxis. An adult patient presents with left ear pain but no hearing loss, beginning 4 weeks ago and partially controlled with narcotic pain medication. A smoking history should be obtained, a neck examination should be performed, and the patient should be referred for upper airway endoscopic examination. An empirical trial of oral antibiotics should be prescribed for presumptive otitis media. An empirical trial of topical antibiotics should be prescribed for presumptive otitis externa. A magnetic resonance image of the brain and temporal bone, with contrast, should be ordered. Answer: A Unexplained unilateral otalgia may be a referred pain from an upper aerodigestive tract lesion. Physical examination of the oral cavity, oropharynx, larynx, and hypopharynx should be performed. Tumors of the upper aerodigestive tract often present with an easily palpable, metastatic lymph node in the neck. Smoking, alcohol use, and human papillomavirus infection are risk factors for head and neck cancer. A patient presents with nasal polyps visible on anterior rhinoscopy and also notes a history of asthma exacerbated by nonsteroidal antiinflammatory drug use. A patient presents to your office with a 4-day history of an upper respiratory infection that has prevented attendance at school. The history suggests chronic infection, and the patient should be given oral antibiotics. The history suggests acute infection, and the patient should be given oral antibiotics. The history is consistent with a viral upper respiratory infection, and symptomatic treatment should be recommended. None of the above Answer: C Several meta-analyses have shown that oral antibiotics or topical antibiotics provide no meaningful improvement in sinusitis during the first 7 to 10 days of treatment. Supportive care is the best option; it should include decongestants, hydration, fever control with antipyretics, and patience in allowing the symptoms to resolve. The patient must keep the tongue protruded and respond to questions by nodding the head or by pointing to names of the tastes written on cards. The anterior two thirds and posterior third of the tongue should be tested separately. Neurologic process of renewal can be affected by nutritional, metabolic, and hormonal states as well as by therapeutic radiation, drugs, and age. For example, with interruption of mitosis by antiproliferative agents, return of normal taste function takes a minimum of 10 days, whereas return to normal olfactory function takes more than 30 days. Diuretics can block apical ion channels on a taste bud, and antifungal drugs inhibit cytochrome P-450dependent enzymes at the level of the receptors. Numerous local conditions, such as colds and allergies, chronic sinusitis, and nasal polyposis, can influence the sense of smell by restricting airway patency. Accidental blows to the head can shear the fine axons of the bipolar olfactory neurons and result in loss of smell. Lesions of the fifth, seventh (chorda tympani), and ninth nerves can lead to disordered taste sensation. Olfactory and gustatory disturbances can serve as important diagnostic signs for focal neurologic lesions. Hallucinations of smell and taste occur in persons with epileptogenic lesions affecting the mesial temporal lobe and insular region, respectively. Finally, olfactory disturbances and hallucinations occur with a number of psychiatric illnesses (particularly depressive illness and schizophrenia). The most frequently encountered causes of loss of smell are local obstructive disease, viral infections, head injuries (Chapter 399), and normal aging (Chapter 25).
© 2025 Adrive Pharma, All Rights Reserved..