General Information about Bimat
Bimat, additionally identified by its generic name bimatoprost, is a medicine used for the treatment of glaucoma, ocular hypertension, and lengthening eyelashes. It belongs to the class of medications called prostaglandin analogs and works by reducing the strain inside the attention. Bimat was first approved by the Food and Drug Administration (FDA) in 2001 for the therapy of glaucoma and ocular hypertension. However, lately, it has also gained popularity for its beauty use in lengthening and thickening eyelashes.
Ocular hypertension is another condition by which the pressure inside the eye is larger than regular however doesn't cause any injury to the optic nerve or imaginative and prescient loss. If left untreated, it can finally lead to glaucoma. Bimat can be used in the therapy of ocular hypertension to minimize back the strain inside the attention and prevent any future problems.
Eyes are thought of to be the window to the world and it is important to take excellent care of them. In recent occasions, eye issues have turn out to be a common well being drawback. One such dysfunction is glaucoma, which is a quantity one explanation for blindness worldwide. In addition, many individuals additionally endure from ocular hypertension, a situation by which the strain inside the eye is greater than normal. These eye circumstances require proper therapy to forestall any harm to the optic nerve and preserve good imaginative and prescient. One of the simplest and broadly used therapies for these eye disorders is Bimat.
Apart from its therapeutic uses, Bimat has gained reputation within the cosmetic world as well. Women all over the world want lengthy and thick eyelashes, as they're thought-about a logo of beauty. Bimat has proved to be a game-changer for these who have thin or sparse eyelashes, as it helps in lengthening and thickening them. It works by growing the expansion part of the eyelash hair and making the lashes seem longer and fuller. Bimat for beauty use can additionally be obtainable within the type of an eyelash serum that is applied every day to the base of the higher eyelashes.
Bimat is a safe and efficient medicine when used as directed by a healthcare professional. However, as with every medicine, there may be some unwanted facet effects, corresponding to delicate irritation or redness in the eye, darkening of the pores and skin around the eye, and increased length and thickness of eyelashes. These unwanted effects are usually delicate and resolve on their very own. It is important to follow the dosing directions and precautions as prescribed by the physician to attenuate the risk of unwanted aspect effects.
Glaucoma is a situation in which pressure builds up inside the attention, damaging the optic nerve and causing imaginative and prescient loss. If left untreated, it might possibly eventually result in blindness. Bimat helps in reducing the strain inside the eye by rising the flow of fluid out of the attention, thereby stopping any additional harm to the optic nerve. It is out there in eye drop kind and is usually applied as soon as a day in the affected eye. Bimat has been proven to be extremely effective in lowering intraocular stress and preventing any development of glaucoma.
In conclusion, Bimat has revolutionized the therapy of glaucoma, ocular hypertension, and beauty enhancement of eyelashes. Its effectiveness and minimal unwanted effects have made it a preferred choice among patients and healthcare professionals. Proper use of this medicine can help in stopping vision loss and achieving beautiful, lengthy eyelashes. However, it is always advisable to consult a well being care provider earlier than using Bimat to ensure its safe and efficient use. Remember, healthy eyes are a present and it's our responsibility to deal with them.
Bimat: A Breakthrough in Eye Care Treatment
In this example 4 medications list bimat 3 ml purchase with mastercard, the patient is given natural hormones; however, they are taken at a time when levels in the body are normally low. Tamoxifen is given to block the actions of estrogen in estrogen-receptor dependent breast cancers (see Chapter 60). From what you learned in Chapter 45, explain their role in treating autoimmune disease. Explain the principal actions of the hormones secreted by the hypothalamus and pituitary gland. Apply the nursing process to the care of patients receiving pharmacotherapy for disorders of the hypothalamus and pituitary gland. The two collaborate to secrete hormones that control the function of the gonads, adrenal glands, thyroid gland, kidneys, and the milk-producing tissues of the breast. The functioning of these two glands serves as the control center that provides integration between the nervous and endocrine systems. This chapter examines drugs that directly affect the functions of the pituitary and hypothalamus. Roughly the size of an almond, the hypothalamus lies in the center of the diencephalon of the brain, just superior to the brainstem. To achieve this, the hypothalamus receives input from numerous vital regions of the nervous system, recognizes imbalances, and makes adjustments to bring the body back to homeostasis. Examples of the multiple and diverse functions of this organ include control of body temperature, thirst, appetite, fatigue, circadian rhythms, anger, and the rate of overall body metabolism. The hypothalamus also controls vital functions of the autonomic nervous system such as heart rate, vasoconstriction, digestion, and sweating. For the purposes of this chapter, only the endocrine functions of the hypothalamus are presented. For the hormones secreted by the hypothalamus, there is only one target organ: the pituitary gland. All hypothalamic hormones travel by the blood a short distance to the pituitary, which lies immediately below the hypothalamus. Upon reaching their receptors, the hypothalamic hormones simply increase or decrease the release of hormones by the pituitary gland. Because of this, hormones from the hypothalamus are called releasing hormones or inhibiting hormones. The major hypothalamic hormones and their actions on the pituitary acromegaly, 1172 gland are given in Table 68. These drugs are discussed in other chapters of this text (see Chapters 60 and 72). From what you learned in Chapter 67, which of the two occurs when a hormone is administered as pharmacotherapy for long periods Although the pituitary gland is often referred to as the "master gland," its function is largely controlled by releasing or inhibiting hormones from the hypothalamus. The pituitary gland is divided into anterior and posterior lobes, which have very different structures and functions. The anterior pituitary gland (adenohypophysis) is comprised of glandular tissue that manufactures and secretes hormones that control major body functions and systems. Four of these are called tropic hormones, a term that refers to the ability of these hormones to regulate the secretory actions of other endocrine glands. The anterior pituitary hormones are synthesized and stored in the pituitary until they receive a message from the hypothalamus. The posterior pituitary gland (neurohypophysis), by contrast, consists of nervous tissue and is basically an extension of the hypothalamus. These hormones are manufactured in the hypothalamus and travel down neurons to the posterior pituitary where they are stored until factors stimulate their release. Oxytocin release is stimulated by touch receptors in the nipples of lactating women. Regulation of hormone levels is an essential function because too little or too much of any of these endocrine secretions can cause profound symptoms. As circulating levels of a hormone rise above normal, a message is sent to the hypothalamus, pituitary, or other endocrine gland to shut down the manufacture and secretion of the hormone. When hormones are administered as drug therapy, they can influence this normal negative feedback mechanism. One of the most important examples of this phenomenon is the negative feedback suppression of the adrenal glands caused by administration of corticosteroid medications. The student should review the information on negative feedback in Chapter 67 before proceeding. Because of the widespread effects of the hormones secreted and controlled by the hypothalamus and pituitary glands, disorders of these glands are quite complex. In general, the pathologies of endocrine glands can be categorized as causing hypofunction or hyperfunction of the particular gland. Pituitary disorders can be the result of tumors, surgery, radiation therapy, infection, injury, infarction (loss of blood supply), or bleeding (hemorrhage) in the area. Congenital defects may also result in absent or impaired function of a hormone, or the lack of an enzyme necessary for hormone production. Dwarfism is associated with normal birth length followed by a slowing of the growth rate. In this context, short stature is defined as well below the fifth percentile for age and gender, or more than two standard deviations below the mean (average) height for age and gender.
As indicated by Gracely et al medicine 02 discount bimat 3 ml,44 if the experimenter has knowledge that only a placebo is administered, this may reduce placebo effects. Furthermore, placebo effects may be induced by cues in the experimental procedures. Levine and Gordon37 showed that placebo analgesia could be induced by a hidden infusion of saline, performed in another room by the experimenter, in the absence of explicit information. When the hidden saline infusions were made by a preprogrammed infusion pump, placebo analgesic responses were not observed. It was concluded that physicians could subtly communicate their expectations of treatment outcome, which, in turn, could influence patient response. It has also been reported that higher physiologic arousal prior to administration of electric shock, compared to arousal measured prior to administration of an aversive tactile stimulus,46 was observed even if no programmed information was available to the subjects prior to the aversive stimulus. A similar finding was reported in Flaten et al,18 where nurses were informed that one group of subjects would receive a small dose of a less-effective painkiller and another group would receive a larger dose of an effective painkiller. In a pre-test prior to administration of the drug and painful stimulation, and before any verbal information was provided to the participants, stress levels were higher in the participants that were about to receive the less-effective medication. Thus, the experimenter should not be informed about which group the research participant belongs to when performing the pre-test as this may modulate pain levels even prior to administration of the placebo. The design is the gold standard in studies of effects of drugs, or other treatments where this design can be applied. The concept of double-blind in studies of placebo effects can, however, mean other things. This form of blinding ensures that the experimenter does not induce a bias in the pain report that may mistakenly be interpreted as a placebo analgesic response. Knowledge of the experimental hypothesis can affect the behavior of the experimenter so that the pain report may differ between the natural history and placebo groups. In the second phase, the conditioning phase, inactive treatment is administered, often a cream applied to the bodily site where the pain is administered, that is followed by painful stimulation where the intensity of stimulation is surreptitiously reduced compared to the pre-test. The placebo treatment is the conditioned stimulus, and the reduced pain after application of the placebo is the unconditioned stimulus. The pairing of the conditioned and unconditioned stimuli gives the impression that the reduced pain is due to the placebo treatment. In the post-test, the cream is again applied in the placebo group to induce an expectation of reduced pain, and both groups receive the same levels of painful stimulation, often the same level as in the pre-test. The participants are often informed verbally that the placebo cream is a powerful painkiller, but in some experiments this information has not been provided and a placebo analgesic response has still been observed after application of the cream. A large reduction from the pre-test to the conditioning phase will generate expectations that the placebo is a powerful painkiller. However, if the pain in the post-test is similar to that in the pre-test there may be a mismatch between the expectation of low levels of pain, and the actual pain experienced. The mismatch could weaken expectations about the analgesic effect of the placebo, and reduce placebo analgesia. Thus, some studies have used a level of painful stimulation in the post-test that is intermediate between the pre-test and the conditioning phase. The advantage of having identical pain stimulations in the pre- and post-test is that it allows for the computation of the Group by Test interaction. This interaction cannot be assessed if pain stimuli are of less intensity in the post-test compared to the pre-test, and only the main effect of Group can be computed. An alternative way of inducing placebo and nocebo responses via classic conditioning has been developed by Colloca and Benedetti. Participants were informed that a green light displayed on a computer screen will indicate activation of the electrode pasted on their middle finger which, in turn, would induce analgesia by virtue of a sub-threshold stimulation. Conversely, a red light will indicate that the electrode is not activated, thus they would experience a red-lightassociated painful stimulus (which serves as control). On the other hand, when you see the red light, then the stimulus to the finger is turned off so that you will feel pain. Participants were informed that a green light displayed on a computer screen indicates activation of the electrode pasted on their middle finger which, in turn, would induce analgesia by virtue of a sub-threshold stimulation. The intensity of stimulation was manipulated to give the experience of analgesia in association with the presentation of a green light during the acquisition phase of conditioning (P = pain; N = no pain). Some studies have asked the subjects to indicate, before the placebo takes effect, their expected pain levels, i. To avoid this problem, some studies have asked subjects to estimate the expected reduction in pain, on a scale from 0 to 100%, prior to administration of the placebo. Others have asked subjects about how much painkillers have reduced pain in the past, as past experiences may determine present expectations towards painkillers. However, correlations between reported previous effects of painkillers and the placebo analgesia observed in the experiment are typically low. However, Bjørkedal and Flaten58 investigated both dimensions by asking subjects after the post-test, how certain they were that they had received a painkiller, and how much they had expected the painkiller to reduce their pain. There were correlations between certainty of having received a painkiller and placebo analgesia, but not between degree of expected pain reduction and actually reduced pain. Although a number of issues important for the study of the field have been identified and solved, at least partly, some methodologic issues are in need of more work. On the other hand, important issues regarding response bias and the design of studies have been clarified. However, the field is developing rapidly, and a chapter on the methodologic issues written in 10 years will likely have many new issues not discussed here. The effect of extended and positive information on pain induced by dental procedures. The effect of experimenter gender on autonomic and subjective responses to pain stimuli. Sensory-decision theory analysis of the placebo effect on the criterion for pain and thermal sensitivity.
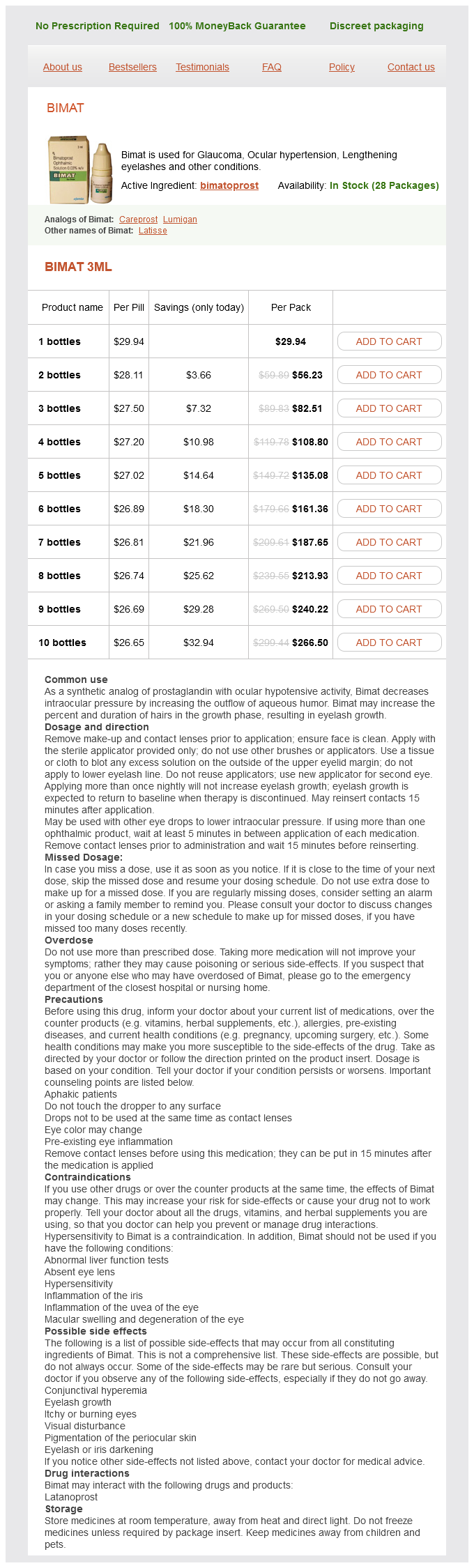
Bimat Dosage and Price
Bimat 3ml
- 1 bottles - $29.94
- 2 bottles - $56.23
- 3 bottles - $82.51
- 4 bottles - $108.80
- 5 bottles - $135.08
- 6 bottles - $161.36
- 7 bottles - $187.65
- 8 bottles - $213.93
- 9 bottles - $240.22
- 10 bottles - $266.50
For each of the classes shown in the chapter outline medicine used during the civil war best order for bimat, identify the prototype and representative drugs and explain the mechanism(s) of drug action, primary indications, contraindications, significant drug interactions, pregnancy category, and important adverse effects. Apply the nursing process to the care of patients who are receiving pharmacotherapy for skin disorders. At times, however, environmental conditions damage the skin, or conditions within the body change, resulting in unhealthy skin. Some of these changes can even lead to systemic changes that affect tissues outside the integumentary system. The purpose of this chapter is to examine the broad scope of skin disorders and the drugs used for skin pharmacotherapy. To understand the actions of dermatologic drugs, it is necessary to have a thorough knowledge of the structure of the skin. The epidermis is the visible, outermost layer that constitutes only about 5% of the skin depth. The middle layer is the dermis, which accounts for about 95% of the entire skin thickness. Some textbooks consider the subcutaneous layer as being separate from the skin and not one of its layers. Each layer of skin is distinct in form and function and provides the basis for how drugs are injected or topically applied. Epidermis: the epidermis consists of epithelial cells with either four or five sublayers depending on its location. The stratum corneum is referred to as the "horny layer" because of the abundance of the protein keratin, a water-insoluble material secreted by keratinocytes, which is also found in the hair, hooves, and horns of many mammals. Keratin gives the skin its tough, protective seal, forming a barrier that repels bacteria and foreign matter. The largest amount of keratin is found in those areas subject to mechanical stress, for example, the soles of the feet and the palms of the hands. The deepest epidermal sublayer, the stratum basale, supplies the epidermis with new cells after older superficial cells have been damaged or lost through normal wear. Over time, these newly created cells migrate from the stratum basale to the outermost layers of the skin. As these cells are pushed to the surface they are flattened and covered with keratin. The outermost skin layer, called the stratum corneum, is composed of these dead cells. On average, it takes a cell about 2-3 weeks to move from the stratum basale to the body surface. Specialized cells within the deeper layers of the epidermis, called melanocytes, secrete the dark pigment melanin. The number and type of melanocytes determine the overall pigment of the skin and determine racial differences in skin tone. Darker skin tones are not caused by an increased number of melanocytes, but by the amount of the pigment melanin that is contained in each cell. In areas where the melanocytes are destroyed, there are milk-white areas of depigmented skin referred to as vitiligo. The junction of the epidermis and the dermis is an area of many ridges and furrows called the rete ridges. It receives its nutrients by diffusion in the rete ridges from the many blood vessels in the dermis. This surface also provides for the ripples seen on the skin surface, which on the fingertips are called fingerprints. Dermis: the second primary layer of skin, called the dermis, is a layer of connective tissue that contains no cells. The dermis is composed of collagen fibers and elastic fibers that give the skin both flexibility and strength. It provides a foundation for the epidermis and accessory structures such as hair and nails. Most sensory nerves that transmit the sensations of touch, pressure, temperature, pain, and itch are located within the dermis, as well as the oil glands and sweat glands. Subcutaneous tissue: Beneath the dermis is the subcutaneous tissue, or hypodermis, which lies over muscle and bone. It consists mainly of adipose tissue, which cushions, insulates, and serves as an energy reserve in the event that extra calories are needed to fuel the body. The amount of subcutaneous tissue varies in an individual and is determined by body area, sex, age, nutritional status, and heredity. Many blood vessels pass through the fatty layer and extend into the dermis, forming capillary networks that supply nutrients and remove wastes. Individual hairs vary in both structure and rate of growth, depending on their location. Composed primarily of dead cells, hair consists of a root that begins in the bulb of the hair follicle and grows from the dermis outward. The hair shaft is the portion that projects through the epidermis and exits the skin. Hair growth occurs in cycles; a growth phase is followed by a resting phase during which hair is shed from the body. The sebaceous glands are distributed over the entire skin surface, except for the palms of the hand and the soles of the feet. Most sebaceous glands are directly connected to the hair follicles; the glands of the eyelids, nipple areolae, and genitalia are freestanding. Sebaceous glands produce sebum, which is emptied into the space between the hair follicle and shaft.
© 2025 Adrive Pharma, All Rights Reserved..