General Information about Arzomicin
Ear infections, also referred to as otitis media, are a typical childhood illness that may additionally affect adults. They happen when the center ear turns into infected and inflamed, inflicting symptoms such as ear pain, fever, and problem listening to. Arzomicin is an effective remedy for ear infections caused by certain micro organism, corresponding to Haemophilus influenzae, Streptococcus pneumoniae, and Moraxella catarrhalis.
Arzomicin comes in various types, together with tablets, oral suspension, and intravenous resolution. The dosage and duration of treatment rely upon the sort and severity of the infection, as properly as the affected person's age and medical history. It is important to observe the prescribed dosage and end the complete course of remedy to ensure full eradication of the an infection and stop the development of antibiotic resistance.
Like all antibiotics, Arzomicin may trigger some unwanted effects, though not everybody will experience them. The most typical unwanted effects embrace nausea, vomiting, diarrhea, and abdomen pain. In rare cases, it may possibly trigger more extreme unwanted effects similar to liver problems, allergic reactions, and listening to loss. It is essential to inform your doctor should you expertise any regarding unwanted effects whereas taking Arzomicin.
Pneumonia, on the other hand, is a more severe an infection of the lungs that could be caused by varied bacteria, viruses, and fungi. It can vary from delicate to severe and even life-threatening if left untreated. Arzomicin is commonly prescribed as a first-line treatment for community-acquired pneumonia as a result of its effectiveness in opposition to Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae.
Aside from respiratory infections, Arzomicin can be used to deal with other bacterial infections corresponding to pores and skin and delicate tissue infections, sexually transmitted diseases, and sure forms of gastrointestinal infections.
In conclusion, Arzomicin (Zithromax) is a highly efficient macrolide antibiotic used to treat a selection of bacterial infections, significantly those of the respiratory tract. It is extensively prescribed because of its broad spectrum of exercise and minimal unwanted effects. However, it may be very important take this treatment as prescribed and notify your doctor of any concerning unwanted aspect effects. With correct use, Arzomicin can successfully deal with infections and improve total health and well-being.
One of the commonest infections Arzomicin is prescribed for is respiratory tract infections, similar to ear infections and pneumonia. It works by inhibiting the growth of micro organism and stopping their capacity to breed, ultimately clearing the an infection and relieving symptoms.
Arzomicin, also identified by its model name Zithromax, is a powerful macrolide antibiotic used to treat a wide selection of bacterial infections. This medicine belongs to the identical class of antibiotics as erythromycin and clarithromycin, however its distinctive chemical structure permits for an extended length of action and a more practical remedy against a variety of bacteria.
Certain precautions should be taken when utilizing Arzomicin. It is not really helpful for patients with a known allergy to macrolide antibiotics or those that have liver or kidney disease. It can also work together with different drugs, so you will want to inform your doctor of some other drugs you're taking.
This lesion affects the central gray structures of the spinal cord with deterioration of alpha-motoneurons and the crossing Neurological Assessment in Spinal Disorders Chapter 11 305 Table 3 can you take antibiotics for sinus infection when pregnant discount arzomicin 500 mg. This syndrome refers to the disturbance of the anterior spinal artery with consecutive affection of the anterior part (bilateral) of the cord. Thus, there is loss of motor function and of sensitivity to pain and temperature (ventrolateral column). This syndrome occurs relatively seldom in trauma and is more frequently seen in non-traumatic disorders (such as B12 deficiency). It produces primarily proprioceptive impairment as a result of impaired posterior column. As a result of a compromise of the conus medullaris (sacral spinal enlargement approximately at the spinal level L1 L2 vertebrae) and/or cauda equina (lumbar nerve roots within the spinal canal), a distinct pattern of bladder-bowel dysfunction and lower limb impairment can be observed. Frequently a clear distinction between conus medullaris and/or cauda equina lesion cannot be achieved. A conus medullaris lesion can present a mixture of flaccid and spastic symptoms of both the bladder and lower limbs depending on the localization within the conus. The extent of symptoms depends on the degree of damage (complete or incomplete) of the conus medullaris and cauda equina. A frequent problem is the differentiation between (Table 4):) central paresis (spastic paresis)) peripheral paresis (flaccid paresis) Differentiation between spastic and flaccid paresis allows the distinction of central from peripheral lesions the differentiation into spastic and flaccid paresis is one of the most significant factors for distinguishing between central and peripheral lesions. A flaccid paresis indicates reduced or abolished muscle tone, while spastic paresis is described by increased muscle tone with resistance to passive extension, brisk jerks and cloni. The muscle resistance is especially present in fast passive extension and at the start of movement. In the presence of spasticity, the muscle tone should be assessed by the adapted Ashworth score (Table 5) [93, 110, 111]. Differentiation of Radicular and Peripheral Nerve Lesions If a peripheral lesion is assumed, differentiation of a radicular and peripheral nerve lesion is required. Differences in the dermatomal area of the roots and peripheral nerves as well as differences in the key muscles may be helpful. However, the sensory examination can be very challenging particularly in elderly and young patients, as well as in patients with impaired consciousness and psychiatric disorders. Also the muscle strength testing depends on the cooperation of the patient and is influenced by pain. The somatotopic relation between nerve root and peripheral nerve is summarized in Tables 6 and 7. Because of the similarity of symptoms, the clinical differentiation between some radicular syndromes and peripheral or plexus lesions can be difficult. Clinical differentiation of central and peripheral paresis Central paresis) brisk tendon reflexes, muscle cloni) uni- or bilateral increased stretch reflexes and enlarged reflex zones) pathological reflexes (Babinski sign, Gordon and Oppenheimer reflexes), uni- and/or bilateral) increased muscle tone) para- or hemi-like distribution of motor deficit) spinal lesions from C1 to L1 (conus medullaris) Peripheral paresis) diminished or absent tendon reflexes) reduced or absent polysynaptic reflexes) no evidence of pathological reflexes) flaccid muscle tone) distribution related to peripheral nerve innervation) lesions below L2 Table 5. Peripheral and segmental innervation of upper extremity muscles Peripheral innervation Muscles of the shoulder trapezius latissimus dorsi rhomboids levator scapulae serratus posterior (superior and inferior) deltoideus supraspinatus infraspinatus teres minor teres major subscapularis Muscles of the arm biceps brachii brachialis coracobrachialis triceps brachii anconeus pronator teres flexor carpi radialis palmaris longus flexor digitorum superficialis flexor carpi ulnaris flexor digitorum profundus flexor pollicis longus pronator quadratus brachioradialis extensor carpi radialis longus extensor carpi radialis brevis extensor digitorum extensor digiti minimi extensor carpi ulnaris extensor pollicis longus extensor indicis longus abductor pollicis longus extensor pollicis brevis supinator muscle Muscles of the hand palmaris brevis abductor pollicis brevis opponens pollicis flexor pollicis brevis adductor pollicis lumbricales abductor digiti minimi flexor digiti minimi brevis opponens digiti minimi palmaris brevis interosseous According to Sobotta [113] Segmental innervation) C3 4) C6 8) C5) C3 5) T1 12) C5 6) C4 6) C4 6) C5 6) C5 6) C5 6) C5 7) C5 7) C5 7) C7 8) C7 8) C6 7) C6 7) C6 7) C7 T1) C8 T1) C8 T1) C8 T1) C8 T1) C5 6) C6 7) C6 7) C6 8) C6 8) C6 8) C6 8) C6 8) C6 8) C6 8) C6) C8 T1) C8 T1) C8 T1) C8 T1) C8 T1) C8 T1) C8 T1) C8 T1) C8 T1) C8 T1) C8 T1) accessory n. Peripheral and segmental innervation of lower extremity muscles Peripheral innervation Muscles of the hip and thigh iliopsoas sartorius quadriceps pectineus adductor longus adductor brevis gracilis obturator externus adductor magnus gluteus maximus gluteus medius gluteus minimus tensor fascia lata piriformis obturatus internus gemelli quadratus femoris Muscles of the leg biceps femoris Segmental innervation) L1 4) L2 3) L2 4) L2 4) L2 4) L2 4) L2 4) L3 4) L2 4) L4 S1) L5 S1) L4 S1) L4 S1) L4 S1) S1 2) L5 S2) L5 S2) L5 S2) S1 3) L5 S2) L5 S2) L5 S2) L4 S1) L4 S1) L4 S1) S1 2) S1 2) S1 2) L4 S1) L5 S1) L5 S1) L5 S1) L4 S1) L4 S1) L5 S1) L5 S1) L5 S1) L5 S1) S2 3) S2 3) S2 3) S2 3) L5 S1) S2 3) S1 2) muscular branch of the lumbar plexus) femoral n. The exact differentiation between radicular and peripheral nerve damage may demand neurophysiological studies, i. Entrapment syndromes are an important differential diagnosis of radicular lesions. C5 Radiculopathy In contrast to an isolated lesion of the musculocutaneous nerve, a C5 lesion causes not only a paresis of the biceps muscle, but also of the scapular muscle Table 8. Frequent entrapment syndromes Syndrome Carpal tunnel syndrome Findings) pain of hand and forearm, frequently at night (antebrachialgia nocturna) hypesthesia of digits 1 to 3 including the radial side of digit 4 paresis and atrophy of the thenar muscles positive Tinnel sign over the carpal tunnel) numbness of digits 4 and 5 paretic intrinsic hand muscles and hypothenar muscles positive Tinnel sign over the ulnar sulcus) paresis of the intrinsic hand muscles worsening of symptoms by elevating the shoulder frequently associated with cervical rip or ligamental hypertrophy pain of hand and forearm) paretic foot elevation numbness of the dorsal foot often history of repeating pressure over the fibular caput) paresis of short foot muscles numbness of the plantar foot atrophy of abductor hallucis muscle Sulcus ulnaris syndrome Thoracic outlet syndrome Fibularis syndrome Tarsal tunnel syndrome group (supra- and infraspinatus, teres major and minor muscles). The sensory deficits of a C5 radiculopathy are located at the posterolateral upper arm while the musculocutaneous nerve also innervates the ventral aspects (see Chapter 8). C6 Radiculopathy the sensory deficits in a C6 lesion may mimic median nerve lesion. Similarly, the middle finger is typically not involved in a C6 hypesthesia but in a median nerve lesion. C8/T1 Radiculopathy this radiculopathy must be distinguished from an ulnar nerve lesion. In C8/T1 radiculopathy, the ulnar side of the forearm is hypesthesic and all intrinsic hand muscles are affected. The ulnar nerve is mostly compressed within the sulcus, resulting in paresis of the hypothenar and only those intrinsic hand muscles innervated by the ulnar nerve. However, detailed testing in femoral nerve neuropathy shows a sensory deficit restricted to the ventral aspect of the thigh with paralysis of hip flexion (iliopsoas muscle) while in L3/4 radiculopathy the sensory deficit is extended to the medial site and below the knee with weakness of the thigh adduction (adductor muscles). L5 Radiculopathy Paresis of foot elevation can be due to a L5 radiculopathy and/or a lesion of the peroneal nerve (see Chapter 8, Case Introduction). Clinical differentiation is Neurological Assessment in Spinal Disorders Chapter 11 311 possible by proving the hip abduction, which is also affected in a L5 radiculopathy with weakness of the gluteal muscles (gluteus medius, tensor fasciae latae). While S1 radiculopathy is signaled by diminished Achilles tendon reflex and weak foot extension, the tibial nerve affection involves the toe and ankle extensor muscles while the peroneal nerve lesion shows paresis of the toe and ankle flexor muscles. Differential Diagnosis of Spinal Cord Compression Syndromes this group of syndromes is due to obliteration of the spinal canal resulting in compression of the neural structures. Both cervical and lumbar stenosis frequently originate from degenerative (secondary) changes of the spine.
Treatment to reduce this fear must include cognitive behavioral techniques that address the perceived threat of movement or pain bacteria en el estomago discount arzomicin 100 mg buy on line, in conjunction with progressive exercise and function. Work-Related Obstacles As outlined in Chapter 21, job satisfaction has been associated with low back pain disability. Similarly, psychological aspects of work such as:) occupational mental stress) general job satisfaction) job related resignation were shown to be related to postoperative relief of disability [26]. Ideally, the rehabilitation process is initiated prior to surgery through a precise and thorough preoperative assessment. Initially an accurate diagnosis is imperative so that the physician can identify an optimal surgical intervention. A thorough physical examination and medical history is useful for identifying comorbidities, since these have the potential to impede the rate of postoperative rehabilitation. This system takes into account function and disability (impairment) with consideration of contextual factors (participation in the activities of daily living, and work and leisure pursuits). Based on the physical and functional assessments, postoperative rehabilitation plans are initiated. The postoperative period can be divided into three phases: Immediate aftercare, rehabilitation and aftercare. Treatment will include transfer and gait training, exercise instruction and education on basic back care. This will continue throughout the inpatient period or until independence is achieved. During this phase patients gradually increase their activities of daily living, the home exercise program continues and all progresses under the guidance of the treating physician. During the aftercare phase, patients are expected to progress further in their functional level both personally and within the occupational and social spheres. Continued exercise is encouraged, both low back stretching and strengthening as well as general aerobic conditioning. To date the existing scientific literature supports exercise after spinal surgery, although no particular form of exercise has been proven optimal. Little exists in the literature describing the ideal postoperative rehabilitation protocol, and common clinical practice is the point of reference. It describes situations with regard to human functioning and its restrictions from a biological, individual and social perspective. Spine 28:209 218 Systematic review of randomized controlled trials about rehabilitation following firsttime lumbar disc surgery. Spine 18:92 97 Randomized controlled trial investigating a high intensity compared to a mild physical rehabilitation program after discectomy. An intensive exercise program appears to increase patient behavioural support and results in work capacity improvements and patient self-rated disability levels. Acta Orthop Scand Suppl 23:2345 2351 A randomized controlled trial demonstrating the advantages of an early active treatment program beginning immediately after lumbar discectomy compared to a less active program. Gejo R, Kawaguchi Y, Kondoh T, Tabuchi E, Matsui H, Torii K, Ono T, Kimura T (2000) Magnetic resonance imaging and histologic evidence of postoperative back muscle injury in rats. Gejo R, Matsui H, Kawaguchi Y, Ishihara H, Tsuji H (1999) Serial changes in trunk muscle performance after posterior lumbar surgery. Hagg O, Fritzell P, Ekselius L, Nordwall A (2003) Predictors of outcome in fusion surgery for chronic low back pain. Manniche C, Asmussen K, Lauritsen B, Vinterberg H, Karbo H, Abildstrup S, Fischer-Nielsen K, Krebs R, Ibsen K (1993) Intensive dynamic back exercises with or without hyperextension in chronic back pain after surgery for lumbar disc protrusion. Curves between 25° and 40° are usually treated with bracing whereas larger curves often are addressed surgically When not treated surgically thoracic curves between 50° and 70° are most likely to progress in adult life Long-term health related quality of life is comparable with non-affected controls but restrictive pulmonary disease may become a serious health problem in thoracic curves larger than 70° the goal of surgery is to prevent curve progression and correct the spinal deformity Surgery usually consists of curve correction and spinal fusion When spinal instrumentation and fusion is indicated, surgical procedures which spare motion segments are favorable the lower lumbar motion segments should be left unfused if possible the reconstruction or preservation of spinal balance is more important than the extent of the curve correction Epidemiology Idiopathic scoliosis is the most common structural spinal deformity in children and adolescents. Scoliosis is defined as a coronal spinal curvature of at least 10° [37] with rotation of the vertebral bodies of unknown origin [36]. About 80 90 % of all idiopathic scoliosis cases develop during adolescence whereas about 10 20 % develop between the age of 3 and 10 years and only about 1 % affect younger patients [179, 184]. The overall prevalence of adolescent idiopathic scoliosis accounts for about 2 3 % in the general population of this age group [97, 204]. Large screening studies of adolescent idiopathic scoliosis revealed incidences of 1. The patient was referred to an orthopedic surgeon, who diagnosed a thoracolumbar curve of 30 degrees with a minor thoracic curve. At the time of referral, the girl was fully active but had some occasional backpain during intensive sports activities. The patient had only recently had her menarche and had been growing rapidly for the last couple of months. The lateral view revealed a flattening of the sagittal profile with a decrease of thoracic kyphosis and lumbar lordosis (b). Surgery was indicated because of a rapidly progressing curve in a patient with a persistent potential for growth. Supine bending films demonstrated a correction of the thoracolumbar curve to 15 degrees (c) and of the thoracic curve to 20 degrees (d). We opted for a short selective anterior fusion by a thoracoabdominal approach because of the still flexible thoracic curve. Six years after surgery, the patient presented with a balanced spine and was symptom free (e).
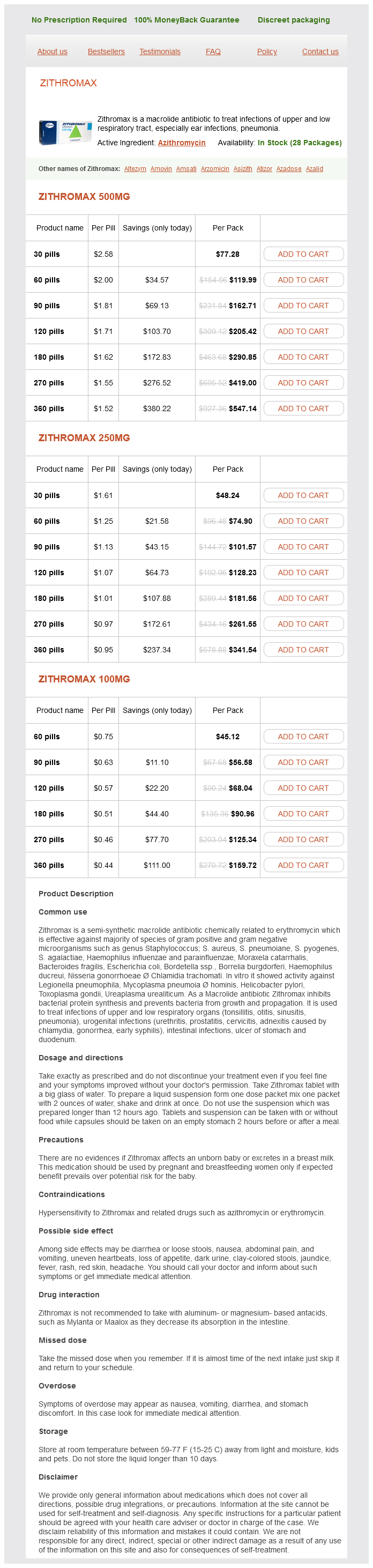
Arzomicin Dosage and Price
Zithromax 500mg
- 30 pills - $77.28
- 60 pills - $119.99
- 90 pills - $162.71
- 120 pills - $205.42
- 180 pills - $290.85
- 270 pills - $419.00
- 360 pills - $547.14
Zithromax 250mg
- 30 pills - $48.24
- 60 pills - $74.90
- 90 pills - $101.57
- 120 pills - $128.23
- 180 pills - $181.56
- 270 pills - $261.55
- 360 pills - $341.54
Zithromax 100mg
- 60 pills - $45.12
- 90 pills - $56.58
- 120 pills - $68.04
- 180 pills - $90.96
- 270 pills - $125.34
- 360 pills - $159.72
Over 90 % of patients coming for spinal fusions that predeposit their own blood avoid receiving allogeneic blood [53] antibiotic resistance report purchase cheap arzomicin line. Iron supplementation with erythropoietin in patients with production problems should be prescribed. Recombinant erythropoietin may substitute blood predeposit Cell Salvage Intraoperative cell salvage consists of collecting the blood from the surgical field to a machine that separates red blood cells from detritus, washing and concentrating them to be reinfused into the patient. Cell salvage is contraindicated in:) infected patients) cancer surgery In a provocative approach, some authors have reinfused collected blood in a large number of cancer patients after irradiation of the bag to kill any malignant cells which are potentially present [25]. More research is needed before recommend- Intraoperative Anesthesia Management Chapter 15 403 ing this approach. Blood collected in the drains within the first 2 4 postoperative hours can also be processed and reinfused with the cell saver system. Pharmacological Measures Tranexamic acid or aprotinin [81] used with the induction of anesthesia has been reported both in adults and children to reduce blood losses in spinal procedures. An increase in coagulability, changes in kaolin/Celite times or severe allergic reactions associated with the use of aprotinin have not been reported with tranexamic acid [26]. Recently, the use of aprotinin was associated with a doubling of the risk of renal failure, a 55 % increased risk of myocardial infarction and a 181 % increase in the risk of stroke in cardiac surgery when compared to tranexamic acid [45]. Desmopressin has not proven useful in decreasing blood losses [76] in idiopathic scoliosis surgery. Blood is separated in blood banks into its components to optimize the use of resources by allowing blood subproducts to be transfused in different patients. The following are recommendations from international publications summarized by Leal-Noval [42] and the American Society of Anesthesiologist Task Force on Perioperative Blood Transfusions 2005 ( The starting dose is 1 unit for 10 kg body weight to increase fibrinogen level by 50 mg % (the hemostatic level is around 100 mg %). A wide range of between 50 and 200 g/kg has been Intraoperative Anesthesia Management Chapter 15 405 advocated. Because of its clearance (35 ml/kg/h), it is suggested to repeat the dose every 2 h in case of persistent hemorrhage [82]. Massive transfusion can be defined as the acute replacement of more than one blood volume within 6 h. Coagulopathy associated with massive transfusion is clinically characterized by the presence of microvascular bleeding or oozing from the mucosae, wound and puncture sites. While thrombocytopenia may develop in massively transfused patients, administration of platelets should be reserved for the patient exhibiting microvascular bleeding and a platelet count of less than 50 000/l. In the massively transfused patient, clinical bleeding associated with coagulation factor deficiencies is unlikely until factor activity levels fall below 20 % of normal. This usually does not occur until greater than one blood volume has been replaced. Whole blood clotting analysis, as seen with thromboelastography, provides a dynamic picture of the entire clotting process. Some potential metabolic problems resulting from blood transfusion are hyperkalemia, hypocalcemia, citrate toxicity, hypomagnesemia, acidosis and impaired oxygen-carrying capacity of hemoglobin. The electrocardiogram should be monitored in all patients for signs of electrolyte abnormality during rapid infusions. Administration of calcium rapidly antagonizes hyperkalemia by promoting transfer of potassium into the cells. Similarly, patients who have sustained an incomplete traumatic spinal cord injury are at risk of further damage. Neurological deterioration can occur because of ischemia of the neural structures secondary to mechanical compression and/or vascular stretching. Monitoring must be performed by an experienced team and the surgeon must be interested in acting on the findings [18]. Teamwork and communication between the electrophysiology technician, anesthesiologist and surgeon are necessary to make spinal cord monitoring useful for the patient. Important facts regarding anesthesia stability and depth, hemodynamics, blood volume, blood flow autoregulation of the spinal cord and temperature must be considered. An elec- Spinal cord monitoring requires clinical practice for its effective use Table 4. Subcortical recordings (from C2) are relatively resistant to the depressing effects seen when cortical level recordings are made. Thiopental is a barbiturate and poses no problems for monitoring neurological parameters during spine surgery after the rapid redistribution of the single induction dose. Short-acting benzodiazepines are combined with opiates or ketamine as part of a balanced technique. Propofol is regarded as a very good alternative for anesthesia during functional monitoring in spine surgery [69]. A 50 % decrease in amplitude and/or a 10 % or 2-ms increase in latency in a hemodynamically stable, normothermic patient are considered as indicators of spinal cord insult [56]. In this case, counteractive measures encompass surgical and anesthetic reactions (see Table 5). Changes in recordings that do not reverse to normal after corrective measures and are still present at the end of the procedure correlate with new postoperative nerve deficits [72]. Repetitive transcranial stimulation (trains of three to five impulses as opposed to a single stimulus) can overcome some of the depressant actions of anesthetics by temporal summation of the descending input on the motoneurons. Partial neuromuscular blockade with continuous and stable infusions of muscle relaxants to keep a train-of-four of 3/4 has been successfully reported [38]. These evoked potentials are large responses clear of signal averaging that can provide the surgeon with good feedback. Some consider there is a malpositioned screw when a recording of compound muscle action potential is obtained of less than 10 mA and 200 s pulse width stimulation.
© 2025 Adrive Pharma, All Rights Reserved..