General Information about Antabuse
It is crucial for patients to grasp that Antabuse isn't a magic tablet that will treatment their alcohol habit. It requires a robust commitment to sobriety and lifestyle modifications to achieve long-term restoration. Some people could expertise side effects from Antabuse, corresponding to drowsiness, complications, or skin rash. It is essential to inform one's physician if these unwanted effects turn into bothersome or severe.
The method Antabuse works is by inhibiting an enzyme referred to as aldehyde dehydrogenase, which is liable for breaking down alcohol in the physique. As a outcome, when an individual takes Antabuse and consumes alcohol, their body is unable to metabolize it properly. This leads to a build-up of a toxic substance referred to as acetaldehyde, which causes a range of unpleasant symptoms such as flushing, sweating, nausea, vomiting, and headache.
If an individual taking Antabuse consumes alcohol, they'll expertise a spread of signs that may final for a number of hours. These symptoms may be dangerous and, in some circumstances, life-threatening, similar to coronary heart palpitations, low blood strain, and issue respiratory. Therefore, it's essential to follow the physician's directions and avoid any alcohol-containing products while taking Antabuse.
Antabuse, also referred to as disulfiram, is a medication used for the remedy of alcoholism. This drug works by causing disagreeable results when alcohol is consumed, which acts as a deterrent for individuals battling alcohol habit. Antabuse doesn't remedy alcoholism, but it might be a helpful device in the recovery process.
Alcoholism is a serious and chronic illness that affects millions of individuals worldwide. It is characterised by a powerful craving for alcohol, an incapability to manage alcohol consumption, and a physical dependence on the substance. Alcoholism can have severe penalties on an individual's health, relationships, and general high quality of life. Therefore, in search of treatment for alcohol habit is crucial for those affected.
Antabuse is prescribed for use as part of a comprehensive treatment program for alcoholism. It is normally mixed with counseling, support groups, and other therapies to address the underlying causes of addiction. This medicine is often used in the first few months of remedy when a person's motivation to remain sober could additionally be at its weakest. It helps build a foundation for sobriety and teaches individuals how to deal with their habit triggers.
Antabuse has been used as a remedy for alcoholism for the explanation that 1940s. It was initially used to deal with parasitic infections, however its effects on alcoholism had been discovered accidentally. Researchers noticed that sufferers skilled adverse reactions after they consumed alcohol while taking the medicine. This led to the development of Antabuse as a therapy for alcohol dependancy.
In conclusion, Antabuse is an effective treatment for people battling alcoholism. It works by causing unpleasant results when alcohol is consumed, which serves as a deterrent for these in recovery. However, it's crucial to keep in mind that this treatment is solely one part of a comprehensive remedy program for alcohol addiction. It requires dedication and a robust dedication to sobriety for people to realize long-term recovery. If you or someone you realize is struggling with alcoholism, search help from a medical professional to debate if Antabuse may be a beneficial remedy possibility.
The worry of experiencing these unpleasant results can be a powerful deterrent for people fighting alcohol habit. Knowing that they will really feel ill in the event that they devour alcohol can help them resist the urge to drink. However, it's important to notice that Antabuse does not deal with the dependancy itself. It merely helps individuals keep sober by making alcohol consumption less desirable.
Certainly medicine 5658 250 mg antabuse overnight delivery, revision surgery is the norm in cases of eyelid involvement and surgeons should prepare patients accordingly for additional procedures which are often required in this population. In nasoethmoid defects without involvement of nasal bones or skin, reconstruction is performed only for dural defects to prevent a cerebrospinal fluid leak. In many cases, the underlying structure can be reconstructed with free tissue transfer, with a traditional paramedian forehead flap offering the optimal skin coverage. As such, the focus becomes providing the bony and soft tissue constructs to support an orbital prosthesis. If resected, it is often necessary to reconstruct the lateral orbital wall to provide a substrate for prosthesis fixation. While reconstruction of critical elements to achieve the traditional goals of maxillary reconstruction is frequently possible, and often highly reliable with free tissue transfer, the sequelae of surgery and 240 30. The current challenges of maxillary reconstructive surgery are not the obliteration of the defect, but center around suboptimal functional and aesthetic subtleties in a large number maxillary ablative defects. Reconstruction of the hard palate using the radial forearm free flap: indications and outcomes. Comparison of functional and qualityof-life outcomes in patients with and without palatomaxillary reconstruction: a preliminary report. Use of the buccal fat pad in the reconstruction and prosthetic rehabilitation of oncological maxillary defects. Osseocutaneous radial forearm free tissue transfer for repair of complex midfacial defects. The radial forearm osteocutaneous "sandwich" free flap for reconstruction of the bilateral subtotal maxillectomy defect. Zygomaticmaxillary buttress reconstruction of midface defects with the osteocutaneous radial forearm free flap. Functional dental rehabilitation of massive palatomaxillary defects: cases requiring free tissue transfer and osseointegrated implants. Maxillary reconstruction can involve a range of options, spanning local and pedicled flaps as well as soft tissue or composite free flaps. Surgical sequelae of maxillary reconstruction of extensive defects often results in suboptimal functional and aesthetic outcomes which require appropriate counseling and often necessitate revision procedures. Microvascular free flap reconstructive options in patients with partial and total maxillectomy defects. Structural pillars of the facial skeleton: an approach to the management of Le Fort fractures. Prosthodontic guidelines for surgical reconstruction of the maxilla: a classification system of defects. A 15-year review of midface reconstruction after total and subtotal maxillectomy: part I. Accuracy and reproducibility of virtual cutting guides and 3D-navigation for osteotomies of the mandible and maxilla. The angular branch of the thoracodorsal artery and its blood supply to the inferior angle of the scapula: an anatomical study. Scapular flap for maxillectomy defect reconstruction and preliminary results using three-dimensional modeling. Scapular angle osteomyogenous flap in postmaxillectomy reconstruction: defect, reconstruction, shoulder function, and harvest technique. Osseointegrated implants: a comparative study of bone thickness in four vascularized bone flaps. Vascularized bone flaps in oromandibular reconstruction: a comparative anatomic study of bone stock from various donor sites to assess suitability for enosseous dental implants. Scapular free vascularised bone flaps for mandibular reconstruction: are dental implants possible Maxillary reconstruction using the scapular tip free flap: a radiologic comparison of 3D morphology. Successful reconstruction of irradiated anterior skull base defect using the dual flap technique involving local pericranial flap and radial forearm free flap. Complications of craniofacial resection for malignant tumors of the skull base: report of an international collaborative study. Reconstruction of lateral skull base oncological defects: the role of free tissue transfer. Usefulness of the anterolateral thigh flap with vascularized fascia lata for reconstruction of orbital floor and nasal surface after total maxillectomy. Beavertail modification of the radial forearm free flap in base of tongue reconstruction: technique and functional outcomes. Byrne Summary the reconstruction of oral cavity defects following cancer resection can prove challenging. The close spatial relationships between distinct tissue types found in the oral cavity can allow invasive malignancies to span multiple subsites. In these cases, reconstructive strategies that restore anatomic form as well as the specialized and coordinated function of each subsite are critical for success. Patient selection, preoperative planning, operative technique, and postsurgical care all greatly influence the ultimate success of multisite reconstruction of the oral cavity. This article will discuss the relevant challenges and potential solutions involved in the repair of these defects. Keywords: oral cavity, carcinoma, squamous cell carcinoma, lip, tonsil, gingiva, palate, tongue, retromolar trigone, buccal, mucosa, salivary gland, pharynx, alveolus, floor of mouth, free flap, skin graft, local flap Evaluation of the patient by the reconstructive team attempts to assess the extent of the disease, predict the anticipated defect, and create a plan for repair.
However medicine 6 clinic discount 250 mg antabuse mastercard, anticonvulsants, especially phenytoin and carbamazepine, both have strong associations with humoral immune deficiency, which may or may not resolve on withdrawal of the drugs. Lamotrigine has been associated with a combined immunodeficiency and opportunist infection. Toxins · Smoking suppresses mucosal immune responses, improving some allergic diseases such allergic alveolitis. Cannabis is particularly dangerous to severely immunocompromised patients as it may contain fungal spores. Thoracic duct drainage · this used to be used as an immunosuppressive technique for the treatment of rheumatoid arthritis. Once normal lymphocyte numbers are achieved, a programme of re-immunization is required, commencing with killed/subunit vaccines. Cardiac surgery in children · Cardiac surgery in children < 2 years old is frequently associated with secondary immunodeficiency ( Physical and environmental factors Radiotherapy and ionizing radiation · Specific immune responses are affected (T and B cells); neutrophil and macrophage function is usually spared unless there is radiation damage to bone marrow. Lymphoedema syndromes A number of familial syndromes have been identified that are associated with lymphoedema. Associated with congenital lower limb oedema, hydrocele, upslanting toenails, papillomatosis, and urethral abnormalities in males. Autosomal dominant, presenting in first two decades with four-limb lymphoedema and varicose veins. Congenital or antenatal onset with generalized severe lymphoedema, lymphangiectasia, learning difficulties, epilepsy, microcephaly, and short stature. Pulmonary manifestations (effusions, chylothorax, pulmonary lymphangiectasia, and pericardial effusions). Proteus syndrome · A hamartomatous condition with partial gigantism of hands and feet, with pigmentary lesions, cerebriform connective tissue naevi, bony abnormalities (hyperostosis and skeletal abnormalities), multiple benign tumours (lipoma, haemangioma) and malignant tumours, capillary and lymphatic vascular malformations, venous thrombosis with pulmonary embolism, and developmental delay. Yellow nail syndrome · rare syndrome of pleural effusions, lymphoedema, and yellow dystrophic nails. Newer administration modes (nanoparticles and biodegradable polymers) are being tested. Polymers of Z variant appear chemotactic to neutrophils so increase recruitment of inflammatory cells. European Guidelines for management exist: · Topical and systemic antibiotics (clindamycin (topical/oral), tetracyclines, rifampicin (with clindamycin). It is clear that there has been an increase in atopic diseases since the Second World War. A reduction in breastfeeding may also have contributed, particularly to atopic eczema. It is also likely that the improvements in public health, leading to elimination in the Western world of parasitic infections, may contribute through a lack of physiological function for the IgEmast cell axis. In the mind of the public, allergy is responsible for all ills but in most cases the blame is wrongly apportioned. Anaphylaxis Anaphylaxis represents the most severe type of allergic reaction and is a medical emergency. Substances causing anaphylaxis Any substance may cause anaphylaxis, but the most common causes are: · venoms: bee and wasp venoms; · legumes: peanuts (and related legumes, soya, and other beans/peas); · true nuts (walnut, almond, cashew, hazelnut, etc. In some cases a cofactor is required for the reaction, such as concomitant aspirin ingestion with the food, or exercise. It is probable that these cofactors alter the amount of allergen entering the circulation. In childhood, sensitization to peanut may occur via formula milk, which may contain peanut oil. Following sensitization, only tiny amounts may be required to trigger subsequent reactions. Activated mast cells also synthesize prostaglandins and leukotrienes, which reinforce the effects on smooth muscle. It is speculative that there are variations in the output of mast cells from bone marrow that influence the possibility of developing reactions. Bradykinin, C3a, and C5a all act as smooth muscle constrictors and increase vascular permeability. Immunological diagnosis · History is all-important, particularly the timing of reaction in relation to the suspected trigger. If the trigger is not clear, a detailed review of all exposures over the preceding 24 hours is required. Measurement of C3a and C5a is possible but requires a special tube, which is unlikely to be available in time. Management of anaphylaxis · 0Immediate management comprises adrenaline (epinephrine) given intramuscularly in a dose of 0. Use hydrocortisone sodium succinate; do not use hydrocortisone phosphate as this is frequently associated with severe burning genital pain, which makes a sick patient feel much worse. It should be reserved for those who have had a systemic reaction and where the risk of further stings is considered to be high. It is important that they tell doctors and dentists as reactions may be triggered during operations by surgical gloves or anaesthetic equipment and by investigations such as barium enema (rubber cuff on tubing) and dental treatment. Indications for prescription of adrenaline for self-injection (EpiPen, Emerade, Jext) · Adrenaline for self-injection should be given when: · patient has had a severe allergic reaction; · there is a risk of re-exposure or the allergen cannot easily be avoided; · patient has had a moderate reaction, but access to rapid medical assistance is impossible; · patient has asthma-reactions are likely to be more severe; Table 3. However, it is recommended that the dose of adrenaline be halved in patients on -blockers, to avoid paradoxical hypertension due to unopposed -adrenergic activity.
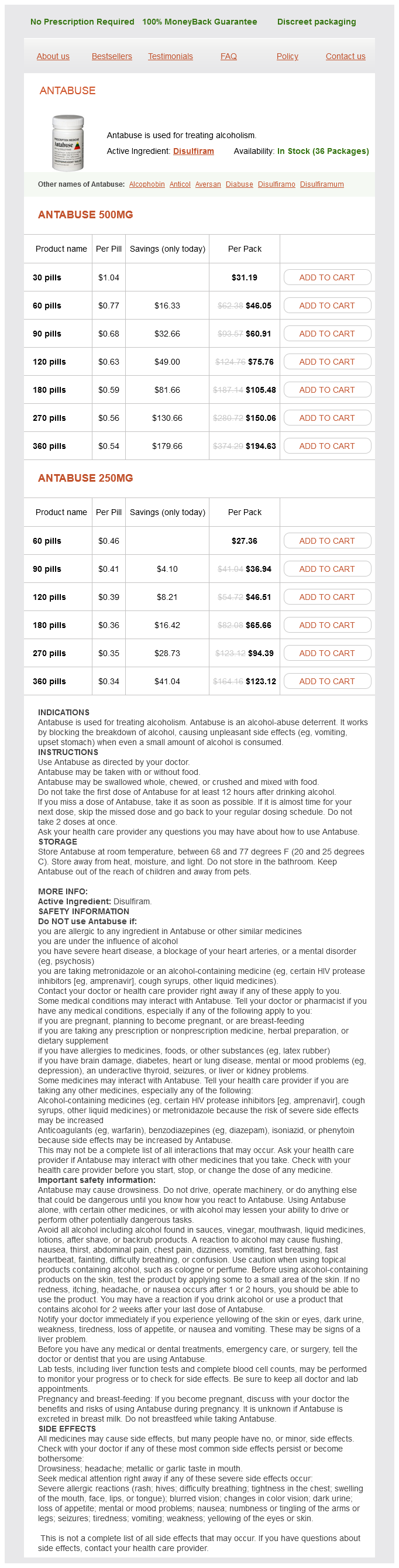
Antabuse Dosage and Price
Antabuse 500mg
- 30 pills - $31.19
- 60 pills - $46.05
- 90 pills - $60.91
- 120 pills - $75.76
- 180 pills - $105.48
- 270 pills - $150.06
- 360 pills - $194.63
Antabuse 250mg
- 60 pills - $27.36
- 90 pills - $36.94
- 120 pills - $46.51
- 180 pills - $65.66
- 270 pills - $94.39
- 360 pills - $123.12
It can also be utilized as an adjuvant treatment after surgical resection or as salvage therapy medicine 3605 generic antabuse 500 mg. Patients with bleeding disorders and multiple medical comorbidities are at higher risk for complications and are not ideal candidates for brachytherapy treatment. In addition, patients with altered mental status that can interfere with treatment compliance are also suboptimal candidates. Patients should be capable of self-care for the duration of brachytherapy treatment, including management of tracheostomy, percutaneous endoscopic gastrostomy or nasogastric tube, and patient-controlled analgesia, as indicated. Patients should have a dental evaluation prior to receiving brachytherapy to fabricate custom dental shields and spacers to shield the mandible from the implant. It offers the unique advantage of directly delivering high doses of radiation locally to tumors while largely sparing surrounding tissues due to rapid dose fall-off. In appropriate setting, brachytherapy offers an organ and functional preservation alternative to surgical resection of oral cavity cancers. It is also a useful technique for local radiation delivery in the adjuvant or salvage settings. It was noted that a small amount of radium left on the skin resulted in ulceration at the site. In 1901, Danlos and Bloch treated nonmalignant skin lesions with local application of unsealed radium sources. Its oncologic application soon followed with the first reported radium treatment for cancer of the palate and pharynx in 1902 in Vienna. Interstitial brachytherapy may be delivered with radioactive sources (typically Ir-192) threaded into catheters temporarily implanted into the tumor volume. Less commonly, it is delivered with permanently implanted radioactive seeds, usually with I-125. Surface mold applicators are commonly used to treat exposed tumors located superficially. The technique of brachytherapy delivery has also evolved from using rigid sources of finite length like in the "Paris System" to employing flexible catheters with the afterloading technique. Paterson and Parker introduced the concept of source loading rules to a single point with the Manchester system for cervical cancer in 1934. Inverse planning allows the planner to generate an idealized plan based on the prescription and dose constraints for the target and organs at risk. The use of geometrical, volume, and inverse optimization forms the basis of optimal planning. Fine tuning to customize clinical target volume coverage versus organ at risk of exposure can be achieved using manual tools that allow manipulation of the dose cloud by the radiation oncologist. Janeway published a series of 24 patients treated from 1915 to 1917 for lip cancer with superficial or deep tissue invasion. Since then, brachytherapy for lip cancer has evolved to include new techniques and technology. Brachytherapy has been employed alone or with external beam radiation as definitive treatment, adjuvantly for positive or close surgical margins, or as salvage treatment. Jorgensen et al reported a large single-institution series of 869 cases of newly diagnosed carcinoma of the lip. Radium needles were inserted transversely and longitudinally into the lesion in the lip. The European Curietherapy Group reported the largest series of 2,363 patients treated for lip cancer from 23 centers. In this multi-institutional report, iridium was found to have improved local control of 96. It is thought that improved dosimetry and implant technique contributed to improved therapeutic efficacy of iridium. Using flexible parallel Ir-192 wires, a mean dose of 65 Gy was delivered for superficial tumors, and 68 Gy was delivered for tumors 5 mm. Increased lesion thickness 1 cm was found to be associated with a higher recurrence rate due to poorer regional control. Guibert et al reported treatment of 92 patients using iridium wires and the Paris system afterloading technique. For interstitial brachytherapy, prophylactic antibiotics are given to decrease the risk of infection at catheter insertion and surgical sites as well as pneumonia. Nutrition during treatment is administered with a nasogastric or gastrostomy tube. A tracheostomy may be necessary to maintain a patent airway and prevent aspiration. Patients should be monitored closely for the duration of brachytherapy treatment to ensure minimal displacement of the catheters and encouraged to ambulate to minimize risk of deep vein thrombosis. During catheter removal, the patient may develop hemorrhage, which can be controlled with bidigital compression while the airway is protected with an inflated tracheostomy cuff. Patients should be discharged with adequate analgesics and appropriate education 275 Brachytherapy for Oral Cavity Cancer Table 34. Patient-reported functional results were satisfactory for 99% of patients, and cosmetic results were satisfactory for 92%. Another modern single-institution series included 89 nodenegative lip cancer cases, 10 after wedge-excision (6 microscopic positive margin, 4 macroscopic residual disease).
© 2025 Adrive Pharma, All Rights Reserved..