General Information about Amaryl
Millions of individuals around the world reside with diabetes, a continual illness that affects the physique's capacity to make use of or produce insulin, which is liable for regulating blood sugar levels. And with the rising prevalence of diabetes, there's a growing want for efficient and accessible therapies. One such treatment is Amaryl, an oral blood sugar-lowering drug from the sulfonylurea class.
In conclusion, Amaryl has been a widely used and trusted therapy possibility for sort 2 diabetes for over 20 years. Its long-acting nature, low risk of hypoglycemia, and helpful results on numerous parameters of glycemic control make it a most well-liked alternative for lots of healthcare professionals. However, you will need to keep in thoughts that Amaryl isn't a standalone therapy for diabetes, and it ought to be used along side life-style modifications to realize optimum results. If you have been prescribed Amaryl, it may be very important follow your doctor's directions fastidiously and regularly monitor your blood sugar levels to ensure its effectiveness in managing your diabetes.
One of some great benefits of Amaryl over different sulfonylureas is its comparatively low threat of hypoglycemia, or dangerously low blood sugar levels. This is as a end result of of its efficiency and its ability to stimulate insulin secretion in a glucose-dependent method. As a end result, it's thought of a safer possibility for elderly patients or those with kidney or liver problems, who are more vulnerable to hypoglycemia. However, you will need to note that hypoglycemia can nonetheless happen if Amaryl isn't taken based on the prescribed dosage and suggestions. Therefore, it is important to observe the instructions of a healthcare skilled while using this medicine.
Amaryl works by stimulating the pancreas to supply extra insulin, thereby increasing the physique's ability to regulate blood sugar levels. This mechanism of action is shared by other sulfonylureas, making it a widely used remedy possibility for kind 2 diabetes. However, what sets Amaryl aside from different similar medicine is its long-acting nature. It has a half-life of about 5-8 hours and a length of action of up to 24 hours, making it a handy once-daily treatment. This reduces the burden of multiple dosing and helps enhance treatment adherence, which is essential for managing diabetes.
Amaryl has a favorable safety profile and is mostly well-tolerated, with the commonest unwanted effects being mild and transient, such as nausea, headache, and dizziness. However, as with any medicine, it might interact with different medicine, so it is necessary to inform your doctor of any other medicines you take before starting Amaryl.
Amaryl, additionally known by its generic name glimepiride, has been used in the treatment of kind 2 diabetes since its approval by the U.S. Food and Drug Administration (FDA) in 1995. It is prescribed for sufferers who have not responded nicely to way of life adjustments such as food plan and train, and who require further help in controlling their blood sugar ranges.
In addition to its blood sugar-lowering effects, Amaryl has also been shown to have other advantages in sufferers with sort 2 diabetes. Studies have shown that it can improve insulin sensitivity, which is a key issue within the development and development of diabetes. It has additionally been linked to reductions in fasting blood sugar levels, post-meal blood sugar spikes, and HbA1c ranges, a measure of long-term glucose management. These benefits contribute to better overall glycemic control, which might help forestall long-term issues of diabetes similar to coronary heart disease, kidney disease, nerve injury, and blindness.
The process of entosis confers the host cells with a competitive advantage over aggressive tumor cells diabetes symptoms hindi amaryl 2 mg line, which can salvage nutrients and amino acids for anabolic reaction via their cannibalistic activity or can increase their genomic instability subsequent to mitotic aberrations. However, inducing entosis by 22 Entosis 471 re-expression of epithelal E- or P-cadherins can reduce the clonogenic potential of breast cancer cells. However, if the effector cell blocks the cytokinesis of the target cells, it can induce the formation of multinucleated or aneuploid target cells. It can also result in chromosome instability, which leads to the further malignancy of target cells through cell fusion. If the target tumor cell with an internalized effector cell is considered as an entity, the killing of internalized cells through entosis can be considered a homeostasis mechanism designed to maintain internal stability [11]. It was noted that some cells in small aggregates appeared to be contained inside large vacuoles, implying their internalization within a neighboring cell. The internalization of one cell within another was observed as early as 6 hours in suspension, and within 12 hours, many of the cells were completely internalized. Cell internalization was initiated approximately 36 hours after detachment and took several hours to complete. In some cases, complex structures resulting from many internaliza tion events were formed, and some cells appeared to reside in a large vacuole following internalization. Internalizing cells were viable and bore into outer cells, suggesting that this process might involve the active invasion of one cell into another. Examination of engulfed cells from 6-hour suspension cultures did not exhibit any apoptotic or necrotic features. Thus, it could be concluded that cell internalization in entosis occurs independent of apoptotic processes. The overexpression of Bcl2 or treatment of cells with the caspase inhibitor had no effect on cell internalization. The addition of phosphatydilserine liposomes, which inhibit phagocytosis, also had no effect on cell internalization. The complex mechanisms that control phagosome maturation up to the point of lysosome fusion are clear. Subsequently, degradation of engulfed cell components occurs, involving the export of digested components and the processing of vacuole membranes. The entotic vacuoles have Rab-7, a late endosome marker, at all sizes, representing different stages of shrinkage; this suggests that vacuoles are in fact hybrid late-endosome/lysosome organelles. Large vacuoles such as phagosomes and entotic vacuoles may therefore continually fuse with lysosomes and at the same time undergo fission in order to maintain lysosome-network homeostasis. Macroendocytic vacuoles formed by phagocytosis, or the live-cell engulfment program of entosis, undergo sequential steps of maturation, leading to the fusion of lysosomes that digest internalized cargo. Phagosomes and entotic vacuoles undergo a late maturation step characterized by fission, which redistributes the vacuolar contents into lysosomal networks. The invading cells in entosis also provide an advantage to the host cell, through nutrient recycling during metabolic stress and starvation. As entosis is involved in eliminating matrix-detached and cancer cells, perhaps inducing it would be therapeutically advantageous and inhibiting it would be detrimental. However, in-depth studies are required to know whether cancer cells have an advantage in escaping entosis, or whether entosis is deregulated in cancers. Entosis is a new phenomenon that requires an implicit definition, and the genetic factors controlling it have to be understood in order to establish its relevance in vivo [5]. The mechanistic elucidation of alternative celldeath mechanisms such as entosis is essential to gaining new insights with major implications for the fields of biology and medicine [13]. E-cadherin is under constitutive actomyosin-generated tension that is increased at cell cell contacts upon externally applied stretch. G-protein-coupled receptor signaling and polarized actin dynamics drive cell-in-cell invasion. Regulation of myosin activation during cellcell contact formation by Par3-Lgl antagonism: entosis without matrix detachment. It has been considered a state that may or may not result in cell death, a distinct case of apoptosis, or a pre-lethal stage [1]. It is currently accepted as a mechanism ensuing from mitotic failure that leads to apoptosis, non-apoptotic cell death, or senescence [2]. Premature mitotic entry is a result of debilitation of the checkpoints responsible for hindering entry into mitosis without damage being repaired first. Once mitosis is underway, the spindle assembly checkpoint ensures that anaphase does not proceed until mitotic spindle formation has occurred properly and chromosomes have secured their bipolar attachment [3]. Upon damage, progression of the cell cycle is halted by these cell-cycle checkpoints. If damage is not repaired, cell-death mechanisms ensue to eliminate the damaged cell [5]. Cells that lack the tumor suppressor p53, for instance as is the case with more than 50% of human solid tumors are deprived of a G2/M checkpoint, and can escape arrest [6]. Such cells can develop mechanisms for surviving in this state and establish abnormal cell populations [6]. For instance, treatment of HeLa cells with etoposide concurrent with Bcl2 suppression did not change the overall clonogenic survival of cells, indicating that although apoptosis was diminished, overall lethality was not [9]. Chromatin 23 Mitotic Catastrophe 477 condensation and chromosome segregation are not completed properly, ensuing giant polyploidy cells that contain decondensed chromatin in multiple micronuclei [3,5].
Therefore diabetes insipidus radiology buy discount amaryl 1 mg on line, it is likely that caspase 11-mediated pyroptosis is required, at least in part, for the restriction of Gram-negative bacteria that access the host cytosol. Notably, this interaction is specific for caspase 8 and not for other caspases. The physiological significance of these observations requires further study, but they suggest that the infectious dose may dictate whether a cell dies a pyroptotic or an apoptotic death. Caspase-1-induced pyroptosis is an innate immune effector mechanism against intracellular bacteria. Horror autoinflammaticus: the molecular pathophysiology of autoinflammatory disease. Differential requirement for Caspase-1 autoproteolysis in pathogen-induced cell death and cytokine processing. Caspase mediated cleavage of phospholipid flippase for apoptotic phosphatidylserine exposure. Panayotova-Dimitrova D, Feoktistova M, Ploesser M, Kellert B, Hupe M, Horn S, et al. Stimulation of Toll-like receptor 3 and 4 induces interleukin-1beta maturation by caspase-8. Inflammatory caspases: linking an intracellular innate immune system to autoinflammatory diseases. Noncanonical inflammasome activation of caspase-4/caspase-11 mediates epithelial defenses against enteric bacterial pathogens. A novel heterodimeric cysteine protease is required for interleukin-1 beta processing in monocytes. Salmonella-induced 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 caspase-2 activation in macrophages: a novel mechanism in pathogen-mediated apoptosis. The interleukin 1beta-converting enzyme, caspase 1, is activated during Shigella flexneri-induced apoptosis in human monocyte-derived macrophages. Caspase-1-dependent pore formation during pyroptosis leads to osmotic lysis of infected host macrophages. Pyroptotic cells externalize eat-me and release find-me signals and are efficiently engulfed by macrophages. Prion-like polymerization underlies signal transduction in antiviral immune defense and inflammasome activation. A novel 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 flow cytometric method to assess inflammasome formation. Caspase-1-dependent processing of pro-interleukin-1beta is cytosolic and precedes cell death. Inflammasome activators induce interleukin-1alpha secretion via distinct pathways with differential requirement for the protease function of caspase-1. Innate immune activation through Nalp3 inflammasome sensing of asbestos and silica. Listeria monocytogenes engineered to activate the Nlrc4 inflammasome are severely attenuated and are poor inducers of protective immunity. Caspase-11 increases susceptibility to Salmonella infection in the absence of caspase 1. Inflammasome-mediated pyroptotic and apoptotic cell death, and defense against infection. Ars Moriendi; the art of dying well new insights into the molecular pathways of necroptotic cell death. In the language of biology, these are translated to mitosis, differentiation, and cell death [1]. The balance between these choices is critical for the development and maintenance of multicellular organisms. There are several types of death, which can be classified based on different characteristics of the cells. The morphological appearance, enzymatic profile, and functional and immunological aspects of the cells are considered in these classifications [2]. With regard to the morphological appearance, three main types of cell death were initially defined in developing tissues, based fundamentally on the role of the lyso somes [3]. Type 3 was nonlysosomal vesiculate degradation, which was further subdivided into two subtypes: type 3A, non-lysosomal disintegration, and type 3B, "cytoplasmic" degeneration. The problem with this classification was that some dying cells showed combined features of more than one of the types, and some seemed not to match any of them [3]. Cell death can also be classified according to enzymological criteria, based on the involvement of nucleases or of distinct classes of proteases, mainly caspases [2]. Hence, "caspase-dependent" and "caspase-independent" cell-death pathways have been pro posed [4]. Usually, cell death is considered to be caspase-dependent when it is inhibited by broad-spectrum caspase inhibitors. Caspase-independent cell death can occur despite the effective inhibition of caspases and with the morphological features of apoptosis, autophagy, or necrosis. Apoptosis does not equal caspase activation, but caspase activation could be a major predictor of death and a defining feature of apoptosis [57]. Some researchers advocate the distinction between developmental/physiological and pathological kinds of cell death. Since many types occur in both situations, any rigid distinction between the two processes should be discouraged. This would also encourage interaction between pathologists and developmental biologists [3]. This was intended to provide uniform and non-rigid nomenclatures that would ensure better understanding and communication among scientists [2]. The first round of recommendations was formulated in 2005 [6] and updated in 2009 [2].
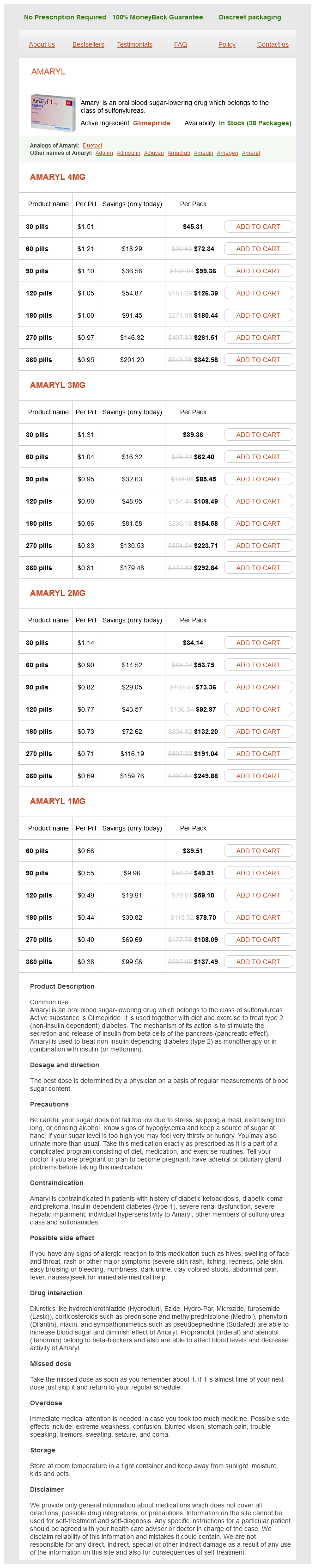
Amaryl Dosage and Price
Amaryl 4mg
- 30 pills - $45.31
- 60 pills - $72.34
- 90 pills - $99.36
- 120 pills - $126.39
- 180 pills - $180.44
- 270 pills - $261.51
- 360 pills - $342.58
Amaryl 3mg
- 30 pills - $39.36
- 60 pills - $62.40
- 90 pills - $85.45
- 120 pills - $108.49
- 180 pills - $154.58
- 270 pills - $223.71
- 360 pills - $292.84
Amaryl 2mg
- 30 pills - $34.14
- 60 pills - $53.75
- 90 pills - $73.36
- 120 pills - $92.97
- 180 pills - $132.20
- 270 pills - $191.04
- 360 pills - $249.88
Amaryl 1mg
- 60 pills - $39.51
- 90 pills - $49.31
- 120 pills - $59.10
- 180 pills - $78.70
- 270 pills - $108.09
- 360 pills - $137.49
Fractures and dislocations should be reduced and splinted in the anatomical position where possible diabetic diet potatoes generic 2 mg amaryl visa, to minimize neurovascular compromise and significant analgesia or procedural sedation may be required to facilitate this. The anatomical position should not be forced if significant resistance is felt. Open fractures should be managed as described in Chapter 23 and the patient referred urgently to an orthopaedic surgeon for definitive management. Significant fractures, open fractures and dislocations may need operative intervention whilst life-saving abdominal or neurological surgery is taking place. They are limbthreatening but not immediately life-threatening, and in the absence of catastrophic bleeding they can be addressed in the secondary survey. Awareness Musculoskeletal injuries occur in 85% of patients sustaining blunt trauma. Major injuries signify significant force applied to the body and so are associated with an increased incidence of chest, abdomen and pelvis damage. Although not immediately life-threatening, they present a potential threat to life and prejudice the integrity and survival of the limb. Crush injuries can lead to compartment syndrome and myoglobin release with the risk of renal failure. These injuries must therefore 690 · Limb injuries are not immediately life-threatening in the absence of catastrophic haemorrhage. Other functions such as protection from the environment, control of body temperature, sensation and excretion can also be harmed. Systemic effects include hormonal alterations, changes in tissue acidbase balance, haemodynamic changes and haematological derangement. Massive thermal injury results in an increase in haematocrit with increased blood viscosity during the early phase, followed by anaemia from erythrocyte extravasation and destruction. Vasoactive substances are released and a systemic inflammatory reaction can result. Inhalational burns Inhalation of super-heated gases and inhalation of toxic smoke in entrapment result in inhalational burns and smoke inhalation. Inhalational injury is now the main cause of mortality in the burns patient, and half of all fire-related deaths are due to smoke inhalation. Direct thermal injury is usually limited to the upper airway above the vocal cords and it can result in rapid development of airway obstruction due to mucosal oedema. Toxic inhalants are divided into three main groups: (1) tissue asphyxiants; (2) pulmonary irritants; (3) systemic toxins. Severe carbon monoxide poisoning will produce brain hypoxia and coma, with loss of airway protective mechanisms, resulting in aspiration that exacerbates the pulmonary injury from smoke inhalation (Table 22. The tight binding of the carbon monoxide to the haemoglobin, forming carboxyhaemoglobin, is resistant to displacement by oxygen, and so hypoxia is persistent. Hydrogen cyanide is formed when nitrogen-containing polymers such as wool, silk, polyurethane or vinyl are burned. Cyanide binds to and disrupts mitochondrial oxidative phosphorylation, leading to profound tissue hypoxia. Burns (thermal, chemical, electrical, cold injury) A burn is a broad term that encompasses not only thermal injury to tissues from heat but injury from electric shock, chemicals and cold. The risk is highest in the 1835 year age group, with a male to female ratio of 2:1 for both injury and death, and serious burns occur most frequently in children under 5 years of age. The last two decades have seen much improvement in burns care, and the mortality rate is now 4% in those treated in specialist burns centres. Circumferential burns around the neck can cause tissue swelling and airway obstruction, and burns around the chest may cause restrictive respiratory failure. They can be subdivided into superficial partial-thickness and deep partial-thickness burns. The deeper layers of the dermis, hair follicles, and sweat and sebaceous glands are spared. Superficial partial-thickness burns heal in 1421 days, scarring is usually minimal, and there is full return of function. There is damage to hair follicles as well as sweat and sebaceous glands, but their deeper portions usually survive. The burned area does not blanch, has no capillary refill and has no pain sensation. Deep partial-thickness burns may be difficult to distinguish from full-thickness burns. Surgical debridement and skin grafting may be necessary to obtain maximum function. Surgical repair and skin grafting are necessary, and there will be significant scarring. Diagnosis of an inhalational burn is made from the history of a fire in an enclosed space and physical signs that include facial burns, singed nasal hair, soot in the mouth or nose, hoarseness, carbonaceous sputum and expiratory wheezing. There is no single method capable of demonstrating the extent of inhalation injury. Stridor is a particularly sinister finding, as it indicates an imminent loss of the airway. Carboxyhaemoglobin levels for carbon monoxide poisoning are useful to document prolonged exposure within an enclosed space with incomplete combustion, as the classically described cherry red skin colour is rare. The chest X-ray may be normal initially; bronchoscopy and radionuclide scanning are useful in determining the full extent of injury. Arterial blood gas analysis will track hypoxia, ventilatory failure and the development of metabolic acidosis. The rule of nines is an approximate tool and tends to overestimate the extent of a burn. Inhalational burns can cause pharyngeal oedema and swelling, which can make tracheal intubation difficult if not impossible.
© 2025 Adrive Pharma, All Rights Reserved..