General Information about Adalat
Adalat is usually well-tolerated by most patients, but like some other medication, it may trigger some unwanted effects. The commonest side effects embrace headache, dizziness, flushing, and swelling of the ankles or ft. These unwanted effects are usually gentle and don't require medical consideration. However, if they persist or turn out to be bothersome, it is essential to seek the assistance of a physician. Adalat may also interact with other medications, so it is important to tell the physician about all the drugs being taken to keep away from any potential interactions.
One of the significant benefits of Adalat is its versatility in treating each hypertension and angina. It is on the market in numerous formulations, including immediate-release tablets, extended-release tablets, and capsules. The immediate-release tablets are taken two to 3 instances a day, while the extended-release tablets and capsules are taken as quickly as a day. This flexibility permits docs to prescribe Adalat in accordance with the person needs of the affected person, leading to higher control of their situation.
Adalat just isn't beneficial for pregnant ladies as it could have adverse results on the fetus. It can also be contraindicated in sufferers with a historical past of coronary heart failure, liver illness, or low blood pressure. It is essential to observe the prescribed dosage and to not stop taking Adalat abruptly, as it might cause a sudden enhance in blood strain.
Adalat, also recognized as nifedipine, is a commonly prescribed medication for the remedy of hypertension (high blood pressure) and angina (chest pain). Since its introduction within the 1970s, Adalat has proven to be an effective and secure choice for managing these situations.
Angina, however, is a type of chest ache that occurs when the heart doesn't obtain enough oxygen. It is a typical symptom of coronary coronary heart illness, which is caused by a buildup of plaque within the arteries. The reduced blood move to the center may find yourself in chest ache, tightness, or pressure. Adalat helps in treating this situation by inflicting the blood vessels to dilate, growing the blood move to the heart and relieving the symptoms.
Hypertension is a continual medical situation characterized by abnormally high blood pressure within the arteries. It is sometimes called a “silent killer” as a result of it could cause harm to the blood vessels and important organs without showing any symptoms until it reaches a important stage. If left untreated, it can result in severe well being issues such as heart attack, stroke, or kidney disease. Adalat works by enjoyable and widening the blood vessels, permitting the blood to move extra easily and lowering the pressure on the guts.
In conclusion, Adalat is a widely used and efficient medicine for treating hypertension and angina. It has a confirmed observe document of being protected and has significantly improved the quality of life for lots of sufferers. With regular monitoring and correct adherence, Adalat can help in decreasing the risk of extreme problems related to high blood pressure and angina. As always, it's critical to seek the guidance of a doctor earlier than beginning any medication and to observe their instructions for the very best outcomes.
Adalat belongs to a class of medicines referred to as calcium channel blockers. It works by blocking the move of calcium into the muscle cells of the guts and blood vessels, which helps to chill out and widen them. This mechanism of motion not solely helps in lowering blood strain but in addition reduces the workload on the guts, making it more effective in treating angina.
Probing structurefunction relations in heme-containing oxygenases and peroxidases arteriogram cpt code discount adalat 30 mg without a prescription. The major genetic defect responsible for the polymorphism of S-mephenytoin metabolism in humans. Formation of glutathionyl-spironolactone disulfide by rat liver cytochromes P450 or hog liver flavin-containing monooxygenases: a functional probe of two-electron oxidations of the thiosteroid Selective phthalate activation of naturally occurring human constitutive androstane receptor splice variants and the pregnane X receptor. Paraoxonase 2 deficiency alters mitochondrial function and exacerbates the development of atherosclerosis. The use of aspirin for primary prevention of colorectal cancer: a systematic review prepared for the U. Net glucuronidation in different rat strains: importance of microsomal beta-glucuronidase. The genetics of alcohol metabolism: role of alcohol dehydrogenase and aldehyde dehydrogenase variants. Use of enzyme inhibitors to evaluate the conversion pathways of ester and amide prodrugs: a case study example with the prodrug ceftobiprole medocaril. An overview of the relations between polymorphisms in drug metabolising enzymes and drug transporters and survival after cancer drug treatment. Enantiomers of thalidomide: blood distribution and the influence of serum albumin on chiral inversion and hydrolysis. Molecular cloning and expression of human liver bile acid CoA:amino acid N-acyltransferase. Drug Interaction Studies-Study Design, Data Analysis, Implications for Dosing, and Labeling Recommendations. In vitro glucuronidation using human liver microsomes and the poreforming peptide alamethicin. Cytochrome p450 enzymes mechanism based inhibitors: common sub-structures and reactivity. Mechanismbased inactivation of cytochrome P450 3A4 by mibefradil through heme destruction. Human cytosolic sulfotransferase database mining: identification of seven novel genes and pseudogenes. The role of decreased gastric alcohol dehydrogenase activity and first-pass metabolism. Evaluation of the characteristics of safety withdrawal of prescription drugs from worldwide pharmaceutical markets-1960 to 1999. Cytochrome P450 gene expression levels in peripheral blood mononuclear cells in comparison with the liver. Contribution of intestinal cytochrome p450-mediated metabolism to drugdrug inhibition and induction interactions. Pregnane X receptor and constitutive androstane receptor at the crossroads of drug metabolism and energy metabolism. Increasing recognition of the importance of aldehyde oxidase in drug development and discovery. A single nucleotide polymorphism in the carboxylesterase gene is associated with the responsiveness to imidapril medication and the promoter activity. Inhibition of urethane-induced carcinogenicity in Cyp2e1-/- in comparison to Cyp2e1 +/+ mice. Species differences in the urinary excretion of the novel primary amine conjugate: tocainide carbamoyl O-beta-D-glucuronide. Use of genetically manipulated Salmonella typhimurium strains to evaluate the role of sulfotransferases and acetyltransferases in nitrofen mutagenicity. Pharmacogenetics of tamoxifen biotransformation is associated with clinical outcomes of efficacy and hot flashes. Explaining interindividual variability of docetaxel pharmacokinetics and pharmacodynamics in Asians through phenotyping and genotyping strategies. Colorectal cancer-specific cytochrome P450 2W1: intracellular localization, glycosylation, and catalytic activity. Amino acid conjugates: metabolites of 2-propylpentanoic acid (valproic acid) in epileptic patients. Role of persistent, non-genotoxic tissue damage in rodent cancer and relevance to humans. Drug-S-acyl-glutathione thioesters: synthesis, bioanalytical properties, chemical reactivity, biological formation and degradation. Characterizing proteins of unknown function: orphan cytochrome P450 enzymes as a paradigm. Glutaredoxin and thioredoxin can be involved in producing the pharmacologically active metabolite of a thienopyridine antiplatelet agent, prasugrel. Stereoselective sulfoxidation of sulindac sulfide by flavin-containing monooxygenases. A novel glutathione transferase (13-13) isolated from the matrix of rat liver mitochondria having structural similarity to class theta enzymes. N-Glucuronidation, a common pathway in human metabolism of drugs with a tertiary amine group. Metabolism and disposition of novel des-fluoro quinolone garenoxacin in experimental animals and an interspecies scaling of pharmacokinetic parameters. The Yc2 subunit is expressed in adult rat liver resistant to the hepatocarcinogen aflatoxin B1. N-Acetylation phenotype and genotype and risk of bladder cancer in benzidine-exposed workers.
A novel pregnane X receptor-mediated and sterol regulatory element-binding protein-independent lipogenic pathway hypertensive urgency guidelines adalat 20 mg online. Structure, function, regulation and polymorphism and the clinical significance of human cytochrome P450 1A2. Substrates, inducers, inhibitors and structureactivity relationships of human cytochrome P450 2C9 and implications in drug development. Inhibition of the catechol-O-methyltransferase-catalyzed O-methylation of 2- and 4-hydroxyestradiol by catecholamines: implications for the mechanism of estrogen-induced carcinogenesis. Activation of the antiviral prodrug oseltamivir is impaired by two newly identified carboxylesterase 1 variants. Recent studies on the structure and function of multisubstrate flavin-containing monooxygenases. The macrolide everolimus forms an unusual metabolite in animals and humans: identification of a phosphocholine ester. Effect of cytochrome P450 polymorphism on arachidonic acid metabolism and their impact on cardiovascular diseases. The basic kinetic concepts for the absorption, distribution, metabolism, and excretion of chemicals in the body system initially came from the study of drug actions or pharmacology; hence, this area of study is traditionally referred to as pharmacokinetics. Toxicokinetics represents extension of kinetic principles to the study of toxicology and encompasses applications ranging from the study of adverse drug effects to investigations on how disposition kinetics of exogenous chemicals derived from either natural or environmental sources (generally refer to as xenobiotics) govern their deleterious effects on organisms including humans. The study of toxicokinetics relies on mathematical description or modeling of the time course of toxicant disposition in the whole organism. The classic approach to describing the kinetics of drugs is to represent the body as a system of one or more compartments, even though the compartments do not have exact correspondence to anatomical structures or physiological processes. These empirical compartmental models are almost always developed to describe the kinetics of toxicants in readily accessible body fluids (mainly blood) or excreta (eg, urine, stool, and breath). This approach is particularly suited for human studies, which typically do not afford organ or tissue data. In such applications, extravascular distribution, which does not require detail elucidation, can be represented simply by lumped compartments. An alternate and newer approach, physiologically based toxicokinetic modeling attempts to portray the body as an elaborate system of discrete tissue or organ compartments that are interconnected via the circulatory system. It also allows a priori predictions of how changes in specific physiological processes affect the disposition kinetics of the toxicant (eg, changes in respiratory status on pulmonary absorption and exhalation of a volatile compound) and the extrapolation of the kinetic model across animal species to humans. It should be emphasized that there is no inherent contradiction between the classic and physiological approaches. The choice of modeling approach depends on the application context, the available data, and the intended utility of the resultant model. Classic compartmental model, as will be shown, requires assumptions that limit its application. In comparison, physiological models can predict tissue concentrations; however, it requires much more data input and often the values of the required parameters cannot be estimated accurately or precisely, which introduces uncertainty in its prediction. We begin with a description of the classic approach to toxicokinetic modeling, which offers an introduction to the basic kinetic concepts for toxicant absorption, distribution, and elimination. This will be followed by a brief review of the physiological approach to toxicokinetic modeling that is intended to illustrate the construction and application of these elaborate models. Finally, we will address the application of toxicokinetic principles to biological monitoring for exposure assessments in industrial and environmental contexts. Serial sampling of relevant biological tissues following dosing can be cost-prohibitive during in vivo studies in animals and is nearly impossible to perform in human exposure studies. The most accessible and simplest means of gathering information on absorption, distribution, metabolism, and elimination of a compound is to examine the time course of blood or plasma toxicant concentration over time. If one assumes that the concentration of a chemical in blood or plasma is in some describable dynamic equilibrium with its concentrations in tissues, then changes in plasma toxicant concentration should reflect changes in tissue toxicant concentrations and relatively simple kinetic models can adequately describe the behavior of that toxicant in the body system. Classic toxicokinetic models typically consist of a central compartment representing blood and tissues that the toxicant has ready access and equilibration is achieved almost immediately following its introduction, along with one or more peripheral compartments that represent tissues in slow equilibration with the toxicant in blood. Once introduced in to the central compartment, the toxicant distributes between central and peripheral compartments. Elimination of the toxicant, through biotransformation and/or excretion, is usually assumed to occur from the central compartment, which should comprise the rapidly perfused visceral organs capable of eliminating the toxicant (eg, kidneys, lungs, and liver). The obvious advantage of compartmental toxicokinetic models is that they do not require information on tissue physiology or anatomic structure. These models are useful in predicting the toxicant concentrations in blood at different doses or exposure levels, in establishing the time course of accumulation of the toxicant, either in its parent form or as biotransformed products during continuous or episodic exposures, in defining concentrationresponse (vs doseresponse) relationships, and in One-compartment model ka guiding the choice of effective dose and design of dosing regimen in animal toxicity studies (Rowland and Tozer, 2011). One-Compartment Model the most straightforward toxicokinetic assessment entails quantification of the blood or more commonly plasma concentrations of a toxicant at several time points after a bolus intravenous (iv) injection. Often, the data obtained fall on a straight line when they are plotted as the logarithm of plasma concentration versus time; the kinetics of the toxicant is said to conform to a one-compartment model. Mathematically, this means that the decline in plasma concentration over time profile follows a simple exponential pattern as represented by the following mathematical expressions: C = C0 e - kel t or its logarithmic transform Log C = Log C0 - kel t 2. Symbols for 1-compartment model: ka is the first-order absorption rate constant, and kel is the first-order elimination rate constant. Symbols for 2-compartment model: ka is the firstorder absorption rate constant in to the central compartment (1), k10 is the first-order elimination rate constant from the central compartment (1), k12 and k21 are the first-order rate constants for distribution between central (1) and peripheral (2) compartment. It can be seen from Equation (7-2) that the elimination rate constant can be determined from the slope of the log C versus time plot (ie, kel = 2. The elimination rate constant kel represents the overall elimination of the toxicant, which includes biotransformation, exhalation, and/or excretion pathways.
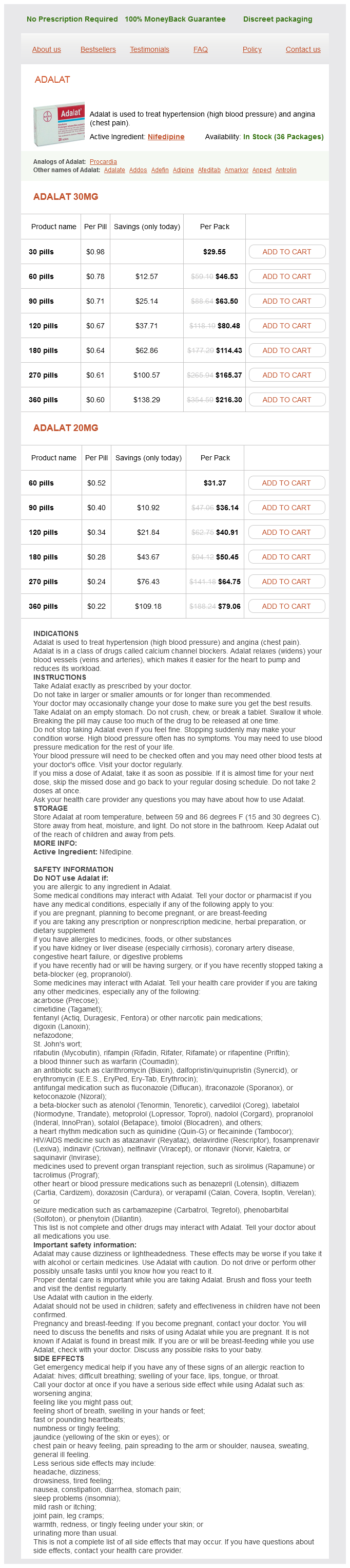
Adalat Dosage and Price
Adalat 30mg
- 30 pills - $29.55
- 60 pills - $46.53
- 90 pills - $63.50
- 120 pills - $80.48
- 180 pills - $114.43
- 270 pills - $165.37
- 360 pills - $216.30
Adalat 20mg
- 60 pills - $31.37
- 90 pills - $36.14
- 120 pills - $40.91
- 180 pills - $50.45
- 270 pills - $64.75
- 360 pills - $79.06
These drugs are nitrogen mustards hypertension benign essential purchase generic adalat canada, which have a tendency to undergo intramolecular nucleophilic displacement to form an electrophilic aziridinium species. In the case of cyclophosphamide and ifosfamide, the nitrogen mustard is stabilized by the presence of a phosphoryl oxygen, which delocalizes the lone pair of nitrogen electrons required for intramolecular nucleophilic displacement. Hydroxylation of the carbon atom next to the ring nitrogen leads spontaneously to ring opening and elimination of acrolein. In the resultant phosphoramide mustard, delocalization of the lone pair of nitrogen electrons to the phosphoryl oxygen is now disfavored by the presence of the lone pair of electrons on the oxygen anion; hence, the phosphoramide undergoes an intramolecular nucleophilic elimination to generate an electrophilic aziridinium species. Rearrangement of trichloroethylene epoxide can be accompanied by migration of chlorine, which produces chloral (trichloroacetaldehyde), or hydrogen, which produces dichloroacetylchloride. Chloral is much less toxic than dichloroacetylchloride; hence, migration of the chlorine during epoxide rearrangement is a detoxication reaction, whereas migration of the hydrogen is an activation reaction. These few examples serve to underscore the complexity of factors that determine the balance between xenobiotic activation and detoxication. As outlined more fully in Point 12 (see the section "Introduction"), the prominence of cytochrome P450 in converting xenobiotics to reactive and potentially harmful metabolites is illustrated by the widespread use of liver microsomes in the in vitro safety evaluation of drug candidates. The concept of "maximum exposure," where 2 perpetrators inhibit 2 parallel pathways of clearance and cause dramatic increases in systemic exposure to the victim drug, was explained in Point 24 in the section "Introduction. Interestingly, the magnitude of the interaction surpasses that predicted from in vitro studies (Obach and Ryder, 2010). The inhibition of dextromethorphan biotransformation by quinidine is a good example of this type of drug interaction. An extensive database on drugdrug interactions is available at the University of Washington Metabolism and Transport Drug Interaction Database. Induction of Cytochrome P450-Xenosensors the induction (upregulation) of xenobiotic-biotransforming enzymes and transporters is a receptor-mediated, adaptive process that augments xenobiotic elimination during periods of high xenobiotic exposure. It is not a toxicological or pathological response, but enzyme induction is often associated with liver enlargement (due to both hepatocellular hypertrophy and hyperplasia), and it may be associated with toxicological and pharmacological consequences, especially for the safety evaluation of drug candidates in laboratory animals and for clinical practice in humans. In animals and humans, enzyme induction may be associated with pharmacokinetic tolerance, whereby the xenobiotic induces its own elimination. Because of autoinduction it is often necessary to increase the dose of carbamazepine at a rate of 200 mg every 1 to 2 weeks to achieve the desired seizure threshold. During safety testing in animals, autoinduction may require increasing dosages of drug candidate to achieve the same degree of systemic exposure. In rodents, lifetime exposure to enzyme inducers may be associated with liver or thyroid tumor formation, as discussed later in this section. In humans, enzyme induction may also be associated with pharmacokinetic tolerance (autoinduction). However, in humans, enzyme induction by one drug (the perpetrator) can augment the clearance of a concomitantly administered drug (the victim), which is a cause of drugdrug interactions. As an underlying cause of serious adverse events, enzyme induction is generally less important than enzyme inhibition because the latter can cause a rapid and profound increase in blood levels of a victim drug, which can cause an exaggerated pharmacological or toxicological effect. In contrast, enzyme induction lowers blood levels, which usually does not cause an exaggerated pharmacological or toxicological response to the drug. Consequently, lack of autoinduction cannot be taken as evidence that a xenobiotic does not cause enzyme induction. Some inducers are potent direct-acting or metabolism-dependent inhibitors such that they mask the activity of one or more of the enzymes they induce. As is the case with all nuclear receptors, the details of the process of activating a xenosensor to its transcriptionally active form are complex and multifaceted. As shown in Tables 6-16 and 6-17, activation of a xenosensor leads to the induction of multiple enzymes, which is called a pleiotypic response. In rodents induction of conjugating enzymes is responsible for increased metabolism of thyroid hormone, which is associated with thyroid follicular cell hyperplasia and tumor formation. Some of the other receptors listed in Table 6-16 are discussed later in this section. However, many species, strain, and individual differences in enzyme induction reflect differences in xenosensor function, as discussed below (this section). The following descriptions of the individual xenosensors focus largely on the mouse and human receptors; studies of the latter have been driven by the desire to investigate drugdrug interactions, whereas studies of the former have been facilitated by the ability to create transgenic mice in which a particular xenosensor has been deleted (so-called knockout or null mice) or replaced with the human receptor (so-called humanized mice). The indole derivative indirubin and indoxyl sulfate, the major metabolite of indole in mammals, and two metabolites of the indoleamine-2,3-dioxygenase pathway, namely, kynurenic acid and xanthurenic acid, are AhR agonists particularly of the human receptor (Omiecinski et al. A notable exception is a class of benzimidazole-containing compounds that includes the proton pump inhibitors omeprazole and lansoprazole. An endogenous AhR ligand is suspected to exist because AhR function is so well conserved from fish to humans and because of developmental abnormalities observed in AhR knockout mice. This process illustrates an emerging role of AhR in the regulation of inflammatory process and liver homeostasis. Exposure of mice to M50367 leads to a decrease in IgE synthesis and peritoneal eosinophilia in allergic experimental models (Negishi et al. The involvement of AhR signaling in tumor invasiveness is further supported by a positive correlation between nuclear localization of the receptor and histopathological characteristics of the neoplasm and long-term survival of urothelial carcinoma patients. This difference further underscores the lack of predictability of rodent data to the human situation. Like metformin, phenobarbital also lowers glucose levels in patients with Type 2 diabetes and improves glucose tolerance and insulin sensitivity in mice (Rencurel et al. Phenobarbital was once used to treat neonatal jaundice, and the Chinese herbal Yin Zhi Huang is still used for this purpose. As the preceding examples in this section illustrate, there is a complex interplay between many of the nuclear receptors listed in Table 6-16. This function of the receptor suggests its role in maintaining liver homeostasis during inflammation. Peroxisome ProliferatorActivated Receptor-Alpha An increase in the size and number of rat hepatic peroxisomes was first observed in response to the hypolipidemic drug, clofibrate.
© 2025 Adrive Pharma, All Rights Reserved..